3156
Highly accelerated sub-millimeter 3D T2 FLAIR based on deep learning and its application in robot-assist PBC for trigeminal neuralgia1Department of Neurosurgery, Clinical Neuroscience Center, Ruijin Hospital, Shanghai Jiao Tong University School of Medicine, Shanghai, China, 2Clinical Neuroscience Center, Ruijin Hospital Luwan Branch, Shanghai Jiao Tong University School of Medicine, Shanghai, Shanghai, China, 3United Imaging Healthcare, Shanghai, China, 4Clinical Neuroscience Center, Ruijin Hospital Luwan Branch, Shanghai Jiao Tong University School of Medicine, Shanghai, China, 5Department of Radiology, Ruijin Hospital Luwan Branch, Shanghai Jiao Tong University School of Medicine, Shanghai, China, 6Central Research Institute, United Imaging Healthcare, Shanghai, China
Synopsis
With 3D T2 FLAIR imaging, trigeminal nerve is clearly demonstrated with CSF nulled, while low SNR and low spatial resolution is always the limitation. In this study, we introduced a 0.75mm isotropic resolution whole brain 3D T2 FLAIR imaging in 5min 40sec based on a novel deep learning framework, and evaluated on a small patient cohort who underwent MR-guided robot-assist percutaneous balloon compression (PBC). To our knowledge, this is the first clinical report of MR-guided robot-assist PBC surgery based on DL accelerated 3D scan.
Introduction
Percutaneous balloon compression (PBC) 1 has been widely used in the treatment of trigeminal neuralgia (TG). At present, most of the surgeries used C-arm fluoroscopy; but observation or identification of the foramen ovale (FO) using conventional fluoroscopy was a challenge. MR guided robot-assist surgery has several advantages such as safety and efficiency 2. Research shows that high resolution MR imaging has the ability to explore the anatomy of the Meckel’s cave 3. With the CSF nulled, 3D T2 FLAIR can clearly demonstrate trigeminal nerve 4 compared with 3D T2 imaging. However, low SNR and long acquisition time hinders its clinical use in PBC.This study implemented a novel deep learning based acceleration framework (AI-assisted Compressed Sensing, ACS) 5 to achieve a highly accelerated 0.75mm isotropic whole brain 3D T2 FLAIR scan in 5min 40sec. We evaluated this imaging technique in MR-guided robot-assist PBC surgery on a small TG patient cohort.
Methods
ACS reconstruction:In this study, we used an extension version of the proposed deep learning based reconstruction framework 5 by replacing 2D kernel with 3D kernel in terms of convolutional neural network (CNN).
MR Scan:
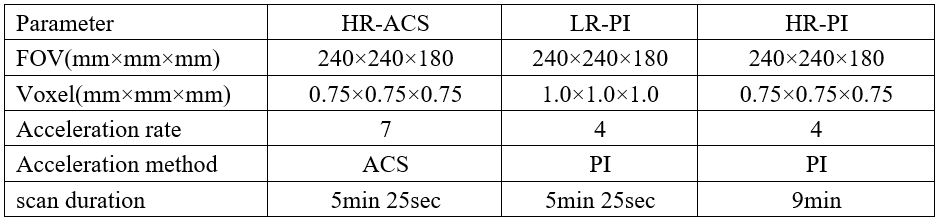
Six patients (two males and four females, median: 65 years old, range: 59–75 years) with TG (symptoms’ duration prior to surgery ranged from 2 to 15 years) underwent MR scan at Ruijin Hospital between August 2021 and September 2021 on a 3.0T scanner (uMR 890, United Imaging Healthcare, Shanghai, China) with a dedicated 64-channel head coil. High resolution 3D T2 FLAIR with ACS is acquired using a 3D MATRIX (Modulated flip Angle Technique in Refocused Imaging with eXtended echo train) sequence (Sagittal plane, FOV: 240×240×180 mm3, voxel: 0.75×0.75×0.75 mm3, acceleration rate: 7, scan duration: 5min 25sec). To evaluate the image quality, the sequence was repeated twice, with only traditional parallel imaging (PI) being turned on and different spatial resolution for comparison. The three sequences were named as HR-ACS (High resolution with ACS), LR-PI (Low resolution with PI), and HR-PI (High resolution with PI). The imaging parameters were listed in table 1.
Surgical procedure:
We utilized the bone fiducials for robot registration and all patients underwent head CT scans after bone fiducials placement. MR and CT data were transferred to a Sinovation planning station (version 2.0.1.2; a portable computer; Sinovation, Beijing, China). The Meckel’s cave was located above the line that connects the puncture entry point in the facial region and the FO in most cases. So our surgical plan included two trajectories. In trajectory A, the entry point was set on the face, and the target point was set on the FO. In trajectory B, the target point was set on the Meckel's cave, and the entry point was set based FO. Sinovation® neurosurgical robot (Sinovation, Beijing, China) was used for puncturing. After surgery, the patients’ symptom relief, BNI pain intensity score and other sensory symptoms were evaluated.
Results
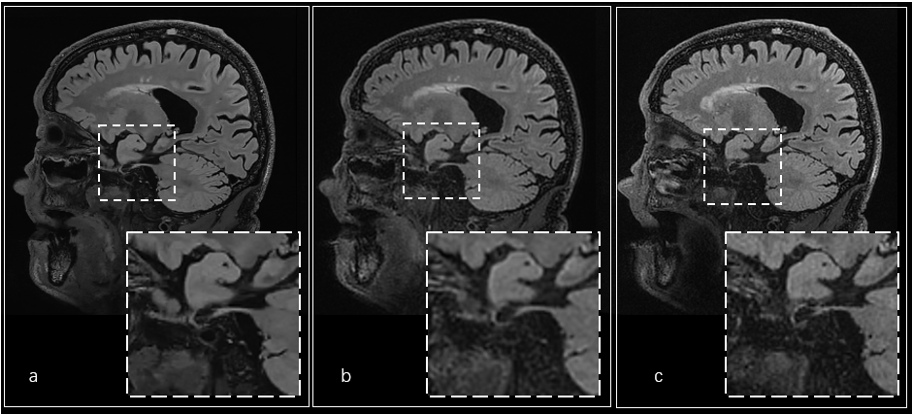
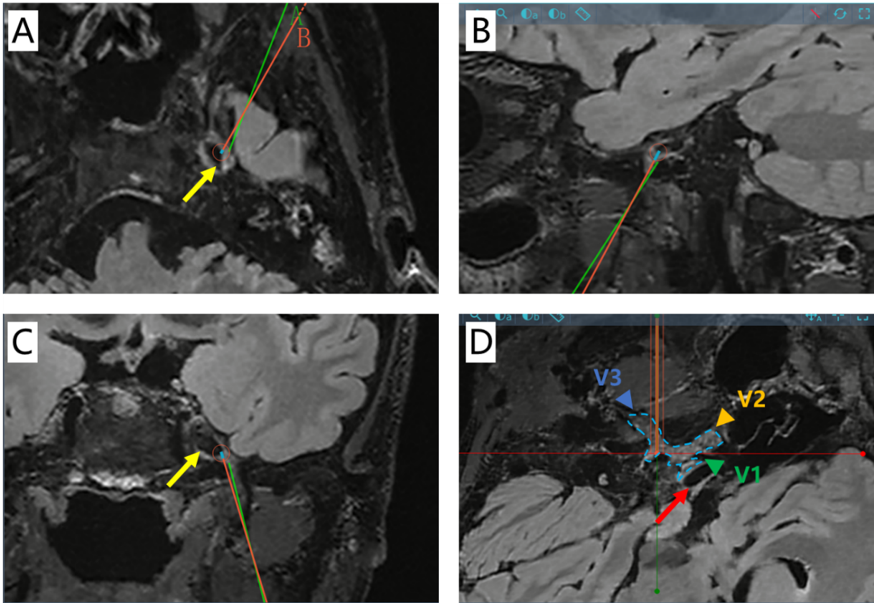
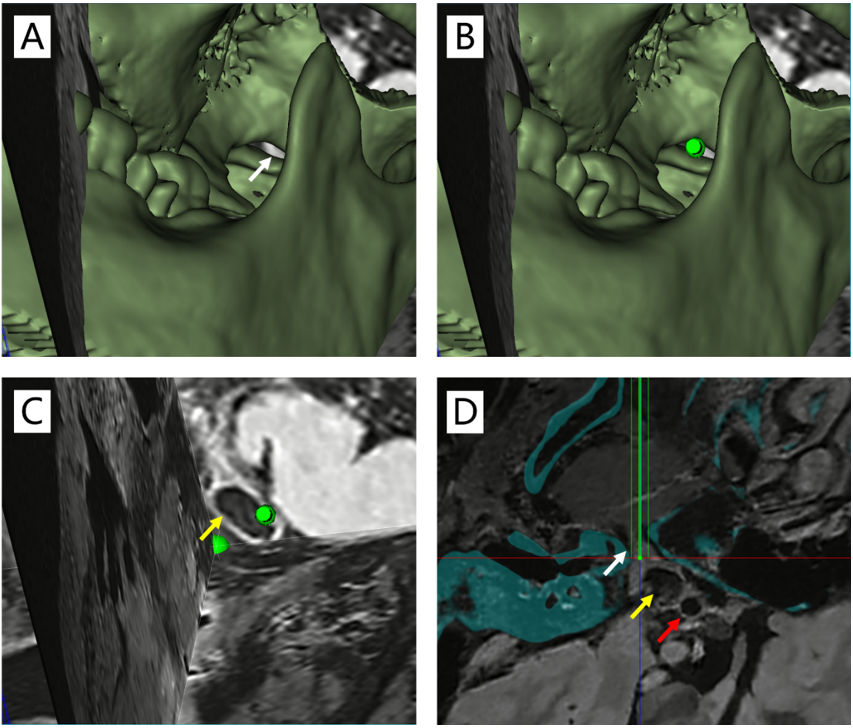
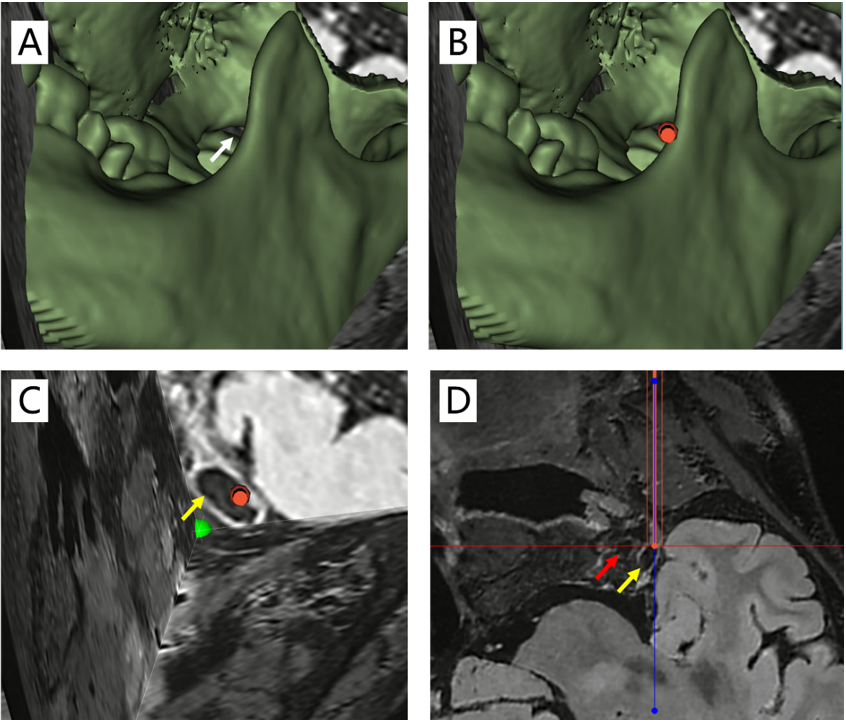
The images from the three sequences were illustrated in figure 1. With the same scan time, HR-ACS achieved higher spatial resolution (0.75 vs. 1.0 mm3) and higher image quality compared with LR-PI. With the same spatial resolution, HR-ACS achieved significant higher image quality and shorter scan duration (5:25 vs. 9:00) compared with HR-PI.In patient images, the Meckel’s cave and the branches of the trigeminal nerve (V1, V2 and V3) could be clearly distinguished (figure 2). All patients underwent puncture according to the trajectory A and B without additional adjustment (figure 3, 4). All patients achieved immediate pain relief following PBC and were classified as having BNI Pain Intensity Score grade Ⅰ. Five patients (83.3%) exhibited facial numbness and facial hypoesthesia, including four cases with BNI numbness score grade Ⅱ and one cases with grade Ⅲ. The sensory symptoms were transient and resolved completely within 3 months following the operation. No permanent or serious complications were encountered in this group.
Conclusions
High resolution 3D T2 FLAIR guided robot-assist PBC is an effective and minimally invasive treatment for TG. MRI can show the location of Meckel’s cave and the branches of the trigeminal nerve, which is conducive to the design of the surgical trajectory and reduces the number of punctures. Neurosurgical robot can accurately achieve the surgical plan and reduce related risks. High resolution DL-based MR imaging and robot-assisted surgical approaches should also be further developed and widely adopted in PBC.Acknowledgements
We sincerely thank the participants in this study.References
1. Mullan S, et al. Percutaneous microcompression of the trigeminal ganglion for trigeminal neuralgia. J Neurosurg. 59(6):1007-1012(1983).
2. Alverdy, J.C. The Benefits of Robotic Surgery: Are They Technical or Molecular?. J Gastrointest Surg 25, 578–580 (2021)
3. Tsutsumi, Satoshi et al. “Meckel Cave: An Anatomical Study Using Magnetic Resonance Imaging.” Journal of computer assisted tomography vol. 45, 5 (2021): 743-748.
4. Jihoon Cha, et al. Trigeminal neuralgia: Assessment with T2 VISTA and FLAIR VISTA fusion imaging. Eur Radiol 21, 2633–2639 (2011).
5. Renkuan Zhai, et al. Intelligent Incorporation of AI with Model Constraints for MRI Acceleration. Proc. Intl. Soc. Mag. Reson. Med. 27 (2021): 1760
Figures