3154
The value of DKI technique in the study of brain Microstructural damage and Cognitive function in patients with OSAHS1Shanxi Medical University, Taiyuan, China, 2The Sixth Hospital of Shanxi Medical University, Taiyuan, China, 3GE Healthcare, Beijing, China
Synopsis
Obstructive sleep apnea hypopnea syndrome (OSAHS) can lead to cognitive dysfunction, and in severe cases, it may develop into dementia. Early, timely and accurate diagnosis is of great significance to delay the progression of the disease, improve the quality of life and improve the prognosis. Diffusion kurtosis imaging (DKI) based on non-Gaussian model to characterize the diffusion of water is regarded as a more sensitive technology to explore the microstructural tissue changes in compare with diffusion tensor imaging (DTI). In this study, the mean kurtosis (MK) from DKI is used to assess the possible abnormality of brain regions in white and gray matter in moderate and severe OSAHS patients. And the correlation between MK values and cognitive function changes was also analyzed. The MK was found to be associated with changes in 9 brain regions including right postcentral gyrus gray matter, parietal lobe gray matter, insular gray matter, left precentral gyrus white matter, frontal lobe white matter and bilateral cingulate gyrus, left occipital lobe gray matter, and well correlated with attention, delayed recall, which can be helpful for understanding of the potential mechanism for neurocognitive function impairment and doing the evaluation.
Introduction
Obstructive sleep apnea hypopnea syndrome (OSAHS) is a common sleep disorder characterized by recurrent apnea or hypopnea caused by obstruction of the upper respiratory tract during sleep, often accompanied by intermittent hypoxemia, sleep fragmentation and so on1. Current studies have shown that OSAHS can damage the neurocognitive function of patients and affect their quality of life2. However, the mechanism of neurological disorder behind its cognitive impairment is not clear, and there were studies speculating that chronic intermittent hypoxia and sleep structure disorder may lead to varying degrees of changes in brain structure, function, metabolism and so on3.At present, there are few DKI studies on OSAHS, and the existing research mainly focuses on the changes of its brain microstructure, not the cognitive function. This study aims to investigate the microstructural changes of brain tissue in patients with OSAHS with DKI imaging and explore the relationship of the mean kurtosis(MK)quantification and the cognitive function of patients with moderate and severe OSAHS.Materials and Methods
27 patients with moderate (15≤ apnea hypopnea index (AHI)<30) and severe (AHI≥30) OSAHS diagnosed by polysomnography (PSG)4 and 27 healthy controls (matched with age, sex and education level) were collected. All the subjects were evaluated with the Montreal Cognitive Assessment scale (MoCA) to get the total score, and subscale scores of visual space and executive function , attention, language and abstraction, delayed recall. Diffusion kurtosis imaging (DKI) (TR/TE=10000/77.4ms,Directions=15/b value,b value=0,1000,2000mm2/s,FOV=24mm,matrix=120×120)and 3D T1-weighted imaging (T1WI) (TR/TE=5.7/2.4ms,FOV=24mm,matrix=224×224) were performed on a 3.0T MR scanner (SIGNA Pioneer, GE Healthcare, Waukesha, WI, USA) for all subjects. The DKI images were processed to generate the MK parametric map by using iQuant software (GE Healthcare, Beijing, China). Then the MK maps were registered to 3D T1WI and deformed to the MNI (Montreal Neurological Institute) space in SPM12 (https://www.fil.ion.ucl.ac.uk/spm/software/spm12/). A customized brain atlas based on the automated anatomical labeling atlas (AAL3, https://www.gin.cnrs.fr/en/tools/aal/) were used to quantify the MK values in each brain regions automatically. IBM Statistical Package for Social Sciences (SPSS v26) was applied for statistical analyses. After the normality and homogeneity of variances were checked, the independent-samples Student t tests, Mann-Whitney U test or χ2 test were used to compare the MK quantification in each brain region between the OSAHS and the healthy control groups. The correlation analysis between MK value, AHI and cognitive score in moderate and severe OSAHS group used Pearson or Spearman correlation analysis. P < 0.05 means the difference with statistically significant.Results
The demographic characteristics of all subjects were shown in Table 1. No significant difference was found in the gender, age, and the years for education between two groups. The MK values were found significant differences in 9 brain regions as shown in Table 2. There were decreased MK values in right postcentral gyrus gray matter, parietal lobe gray matter, insular gray matter, left precentral gyrus white matter, frontal lobe white matter and bilateral cingulate gyrus, while increased MK values in the left occipital lobe gray matter. Correlation analysis (table3) showed that the MK value of left frontal lobe (r = 0.480, P <0.05) and parietal lobe white matter (r = 0.727, P <0.05) in OSAHS group was negatively correlated with AHI. The gray matter of right insular lobe (r = 0.482, P < 0.05), white matter of left precentral gyrus (r = 0.572, P < 0.05), white matter of parietal lobe (r = 0.626, P < 0.05) and white matter of frontal lobe (r = 0.491, P < 0.05) were positively correlated with attention, and the gray matter of right parietal lobe was positively correlated with delayed recall (r = 0.465, P < 0.05).Discussion
In this study, it was found that the MK value of white matter of left frontal lobe and parietal lobe decreased with the severity of OSAHS. We speculate that intermittent hypoxemia and sleep fragmentation may lead to damage of white matter integrity and loss of gray matter by mediating pathological processes such as hypoperfusion, endothelial dysfunction and neuroinflammation.Correlations between some brain regions (right parietal cortex, right insular cortex, left parietal WM, left frontal WM, left central anterior gyrus white matter) and their sub-scores (attention and delayed recall) were found, but not between the MK in brain regions and MoCA total scores, indicating that the changes of cognitive function in patients with OSAHS were mainly manifested in different degrees of delayed recall, attention impairment. Previous studies have found that the parietal cortex is involved in the storage and retelling of working memory, patients with impaired right inferior parietal cortex have impaired spatial processing and memory5, as confirmed by the results in our study. The frontal and parietal white matter fiber bundles undertake the integration and processing of brain information. Parietal and frontal white matter constitute most of the entire brain white matter fibers, which explain that the pathological changes in this area have a greater impact on cognition. This may be the reason for the impaired attention of OSAHS patients.
Conclusions
Mk values of DKI imaging are associated with the microstructural changes in brain regions of patients with moderate and severe OSAHS, and could be useful biomarker for evaluating the impairment of cognitive function.Acknowledgements
The authors acknowledge grant support from The Sixth Hospital of Shanxi Medical University and GE Healthcare.References
1. Veasey SC,Rosen IM. Obstructive Sleep Apnea in Adults[J]. N Engl J Med,2019,380(15):1442-1449.
2. Seda G,Han TS. Effect of Obstructive Sleep Apnea on Neurocognitive Performance[J].Sleep Med Clin,2020,15(1):77-85.
3. Baril AA, Martineau-Dussault MÈ, Sanchez E, et al. Obstructive Sleep Apnea and the Brain: a Focus on Gray and White Matter Structure[J]. Curr Neurol Neurosci Rep,2021,21(3):11.
4.Khurana S, Soda N, Shiddiky MJA, et al. Current and Future Strategies for Diagnostic and Management of Obstructive Sleep Apnea[J]. Expert Rev Mol Diagn. 2021,8.
5.Hideya Koshino,Patricia A,Nancy,et al.Functional connectivity in an fMRI working memory task in high functioning autism[J].Neuroimage,2005,24(3):810-821.
Figures
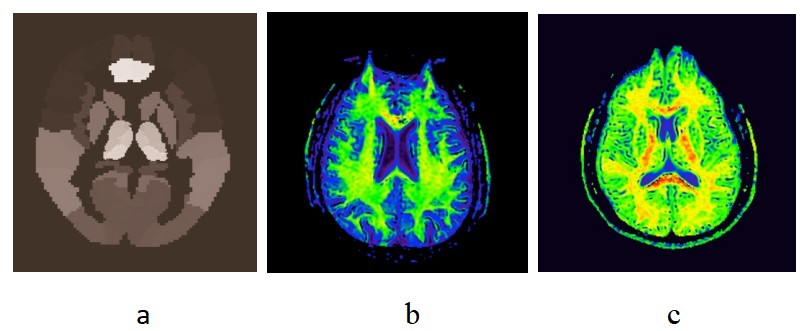
Table 1 Demographic characteristics of OSAHS patients and healthy controls
Table 2 The MK values in brain regions with significant differences between the OSAHS and the healthy control group
Table 3 Correlation analysis between the MK quantification in brain regions and the scores of cognition evaluation in OSAHS patients
Figure 1 The atlas (a)and representative MK parameter maps for a OSAHS(b) patient and a healthy control(c)