3144
Comparison of Ultrashort Echo Time MRI with High-Resolution CT for the Assessment of Idiopathic Pulmonary Fibrosis
Xiaoyan Yang1, Min Liu1, Jing An2, Thomas Benkert3, Huaping Dai1, and Chen Wang1
1China-Japan friendship hospital, Beijing, China, 2Siemens Shenzhen Magnetic Resonance Ltd., Shenzhen, China, 3Siemens Healthcare GmbH, Erlangen, Germany
1China-Japan friendship hospital, Beijing, China, 2Siemens Shenzhen Magnetic Resonance Ltd., Shenzhen, China, 3Siemens Healthcare GmbH, Erlangen, Germany
Synopsis
This study investigated the feasibility of ultrashort echo time (UTE)-MRI to evaluate the radiologic findings of idiopathic pulmonary fibrosis, using high resolution CT (HRCT) as the reference standard. UTE-MRI is inferior to HRCT in identifying the details of lung parenchyma. The results suggest that UTE-MRI is equivalent to HRCT. In addition, inter-method agreement between UTE-MRI and HRCT were equal to inter- and intra-observer agreement for UTE-MRI for evaluating disease findings. Moreover, performance analyses demonstrated that UTE-MRI efficacy for detecting radiologic findings of pulmonary fibrosis, such as reticulation, traction bronchiectasis, and honeycombing were similar to that of HRCT.
Introduction
Idiopathic pulmonary fibrosis (IPF) is a chronic progressive fibrosis disease of the lung with a poor prognosis and median survival of 3-5 years from diagnosis. High-resolution CT (HRCT) yields images with excellent anatomic detail of the lung and plays a key role in the management and differential diagnosis of IPF. However, radiation exposure is a significant concern in patients with IPF during longitudinal follow-ups. Thus, a radiation-free imaging tool is desirable. Recently, MRI with ultrashort echo time (UTE-MRI) sequences were applied for quantitative and qualitative assessment of lung parenchymal changes 1, 2. UTE-MRI image quality was comparable with that of HRCT 3. The aim of this study was to assess the utility of UTE-MRI for lung parenchymal imaging and compare the result with that of HRCT to diagnose IPF.Methods
Following informed consent, a total of 36 patients (men: 34 (94.4%), women: 2 (5.6%); mean age: 62, age range: 43-78) were enrolled in the study. All patients underwent HRCT and MRI examinations. HRCT was obtained with multi-slice spiral CT scanners (Brilliance CT, Phillips Healthcare, Netherlands; Toshiba CT, Tokyo, Japan). UTE-MRI was performed with a 1.5T system (MAGNETOM Aera; Siemens Healthcare, Erlangen, Germany) during free-breathing. A prototypic 3D UTE sequence with a stack-of-spirals trajectory was used for data acquisition4 repetition time=3.85 msec; echo time=0.05 msec; flip angle=5°; voxel size=1.5 x 1.5 x 1.5 mm3). Free-breathing was enabled by prospective gating. Here, respiratory information was provided by a navigator and scanning is automatically stopped once sufficient data was acquired in end-expiratory state. Corresponding scan times depended on the breathing pattern and was within the range of 6-7 minutes. According to preoperative findings, the image quality of both HRCT and MR images was estimated using a 5-point scale. To compare the ability of UTE-MRI to assess lung parenchymal characteristics with HRCT, a 2-point visual scoring system was used to determine the presence of reticular and honeycombing patterns, traction bronchiectasis, and ground-glass opacities 5. The extent of interstitial lung changes was graded on a system according to Gay et al. 6. Two radiologists evaluated HRCT and MRI images independently for various morphologic abnormalities associated with IPF. The difference in image quality between HRCT and UTE-MRI was compared using a Wilcoxon-rank sum test. Kappa and weighted kappa analyses were used to measure intra- and interobserver, and inter-method agreements. Sensitivity and specificity were used to assess the performance of UTE-MRI for detecting pulmonary fibrosis.Results
A representative case of IPF is shown in Figure 1. All interobserver agreements for image quality were statistically significant (HRCT: k=0.786; P<0.0001; UTE-MRI: k=0.719; P<0.0001). As Figure 2 shows, the mean image quality score for HRCT (4.9±0.3) was significantly higher than for UTE-MRI (4.1±0.7; P<0.0001). Moreover, the inter-observer agreements of HRCT and UTE-MRI for the ability to detect the imaging characteristics of IPF were defined as substantial and excellent, respectively (HRCT: 0.727≤k≤1, P<0.0001; UTE-MRI: 0.719≤k≤0.824, P<0.0001). In addition, reticular (97.1%, k=0.654) and honeycombing (83.3%, k=0.625) patterns, and traction bronchiectasis (94.1%, k=0.640) were well visualized on UTE-MRI. For an IPF diagnosis, the sensitivity of UTE-MRI was 97.2%. The UTE-MRI protocol could diagnose IPF in 28 (90%) of 31 patients, with a total fibrosis score of 6-15, and 2 (40%) of 5 patients with a total fibrosis score >15. There was excellent interobserver agreement (HRCT, k=0.873, MRI, k=0.920).Discussion & Conclusion
CT is considered an accurate tool to image lung parenchyma with excellent structural detail. However, the major disadvantage is ionizing radiation exposure; thus, an alternative radiation-free imaging modality is needed, particularly in certain patient groups, as well as in longitudinal studies. In this study, our results suggest that UTE-MRI is not significantly inferior to HRCT and has a similar potential to detect the radiologic characteristics of IPF and make a diagnosis. In addition, UTE-MRI is useful for sampling free induction decay using short repetition times that limit signal contaminations from long T1 signals and low proton density components, such as the lung parenchyma 7. In conclusion, UTE-MRI could be used in routine clinical practice as a radiation-free imaging modality in patients with IPF.Acknowledgements
No acknowledgement foundReferences
1.Bauman, G, Johnson, KM, Bell, LC, et al. Three-dimensional pulmonary perfusion MRI with radial ultrashort echo time and spatial-temporal constrained reconstruction. Magn. Reson. Med. 2015; 73(2):555-564 2.Ma, W, Sheikh, K, Svenningsen, S, et al. Ultra-short echo-time pulmonary MRI: evaluation and reproducibility in COPD subjects with and without bronchiectasis. J. Magn. Reson. Imaging. 2015; 41(5):1465-1474 3.Dournes, G, Grodzki, D, Macey, J, et al. Quiet Submillimeter MR Imaging of the Lung Is Feasible with a PETRA Sequence at 1.5 T. Radiology. 2015; 276(1):258-265 4.Cha, MJ, Park, HJ, Paek, MY, et al. Free-breathing ultrashort echo time lung magnetic resonance imaging using stack-of-spirals acquisition: A feasibility study in oncology patients. Magn. Reson. Imaging. 2018; 51:137-143 5.Lynch, DA, Sverzellati, N, Travis, WD, et al. Diagnostic criteria for idiopathic pulmonary fibrosis: a Fleischner Society White Paper. The Lancet. Respiratory medicine. 2018; 6(2):138-153 6.Gay, SE, Kazerooni, EA, Toews, GB, et al. Idiopathic pulmonary fibrosis: predicting response to therapy and survival. Am. J. Respir. Crit. Care Med. 1998; 157(4 Pt 1):1063-1072 7.Jakob, PM, Hillenbrand, CM, Wang, T, et al. Rapid quantitative lung (1)H T(1) mapping. J. Magn. Reson. Imaging. 2001; 14(6):795-799Figures
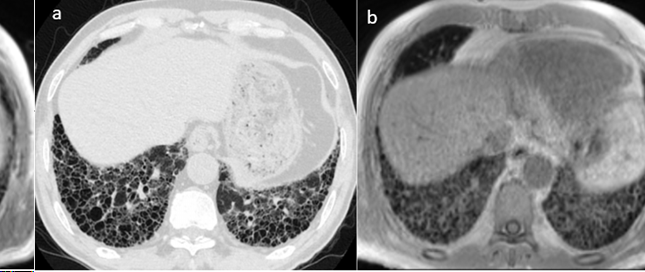
Figure 1. A 77-year-old
male patient with IPF. Images obtained with HRCT (a), and UTE-MRI (b) show
honeycomb and reticular patterns in both the left and right lower lobes.
UTE-MRI and HRCT image quality is equal (image quality score [IQS]: 5). The
extent of pulmonary fibrosis on images obtained with UTE-MRI (IQS: 16) was
equal to those obtained with HRCT (IQS:16).
HRCT, High resolution
CT; IPF, idiopathic pulmonary fibrosis; UTE-MRI, ultrashort echo time MRI
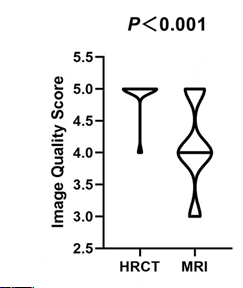
Figure 2. Image quality
scores of HRCT and UTE-MRI.
HRCT, high resolution
CT; UTE-MRI, ultrashort echo time MRI
DOI: https://doi.org/10.58530/2022/3144