3114
Changes of brain function in patients with type 2 diabetes by different analysis methods: A new coordinate based meta-analysis of neuroimaging1Hospital, Fourth Military Medical University, 569 Xinsi Road, Xi’an 710038, Shaanxi, China, Xi’an, China
Synopsis
Neuroimaging meta-analysis have identified abnormal neural activity alterations involved in type 2 diabetes mellitus (T2DM) patients, but there is no consistency and heterogeneity analysis between different brain imaging processing strategies. For the indicators obtained from varied post-processing methods reflect different neurophysiological and pathological characteristics, we further conducted a coordinated-based meta-analysis (CBMA) for two categories of neuroimaging literature grouped by similar data processing indicators. Compared to healthy controls, T2DM patients showed a significantly decreased brain activity in the right rolandic operculum, right supramarginal gyrus and right postcentral gyrus, providing a new non-invasive biomarker for T2DM neuropathy.
Introduction
China has the highest diabetic population, with a prevalence of 12.8% [1]. Type 2 diabetes mellitus (T2DM) accounts for more than 95% of diabetes cases in China, and can lead to cognitive decline and emotional disorders [1, 2]. Reports have shown that a quarter of T2DM patients suffer from mild cognitive impairment (MCI) and progress to dementia at a rate of 8.7% per year [3]. Besides, T2DM patients may got diabetes-related neuropsychiatric diseases, such as depression, anxiety, and panic, etc., which may progress to depression in the future [4, 5]. These disorders severely affect the life quality of T2DM patients [6]. Therefore, it is necessary to assess the neural injury of T2DM, so as to provide a theoretical basis for effective intervention to delay disease progression. We conducted a new meta-analysis using the more reliable and accurate algorithm combing the permutation of subject images (PSI) and Seed-based d Mapping (SDM) software in two groups by different processing methods [7-9], separately reflecting the relationship of neural activity in the brain and the intensity of neural activity [9-11]. This study provides a precise neurobiological mechanism of T2DM causing MCI and can help identify potential early diagnosis and intervention biomarkers.Methods
The study was performed according to the standards of Reporting Items for Systematic Reviews and Meta-Analysis (PRISMA) and ten simple rules for neuroimaging meta-analysis [12, 13]. The protocol for this neuroimaging meta-analysis was registered on PROSPERO (CRD42021247071) (https://www.crd.york.ac.uk/prospero/). Coordinate-based meta-analysis (CBMA) was a widely used method [14], and we further used a new voxel based algorithm of the Seed-based d Mapping (SDM) with the permutation of subject images (PSI-SDM version 6.21, https://www.sdmproject.com) (Albajes-Eizagirre et al. 2019). This more reliable and accurate algorithm can better control the false positive rate and analyzed more information. (Albajes-Eizagirre et al. 2019). We summarized the abnormal brain activity in T2DM and explored whether there were differences between separate meta-analysis and combined meta-analysis on different processing methodology of brain function. Significant peak coordinates were extracted from literature. Peak coordinates not in MNI space were converted using coordinate mapping software. Extracting t value, z value and p value could be converted into t value through https://www.sdmproject.com/utilities/?show=Statistics [15]. Seven standard steps were preformed according to the guideline of the PSI-SDM software: 1) Global analysis; 2) Pre-processing; 3) Mean analysis; 4) Threshold analysis; 5) FEW (family wise error) correction; 6) Threshold analysis; 7) Extract and Blas Test.Results
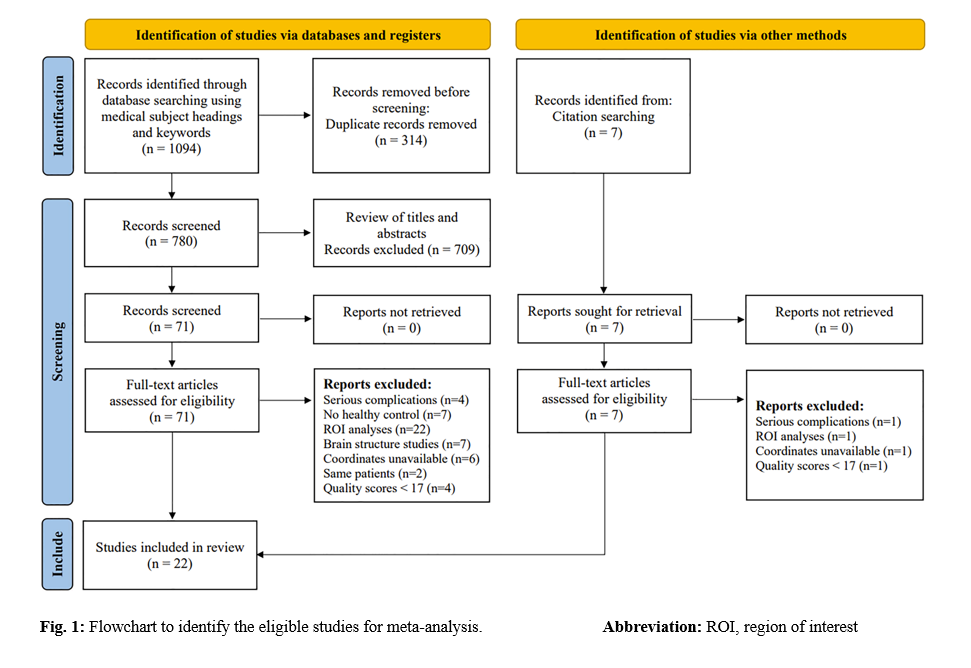
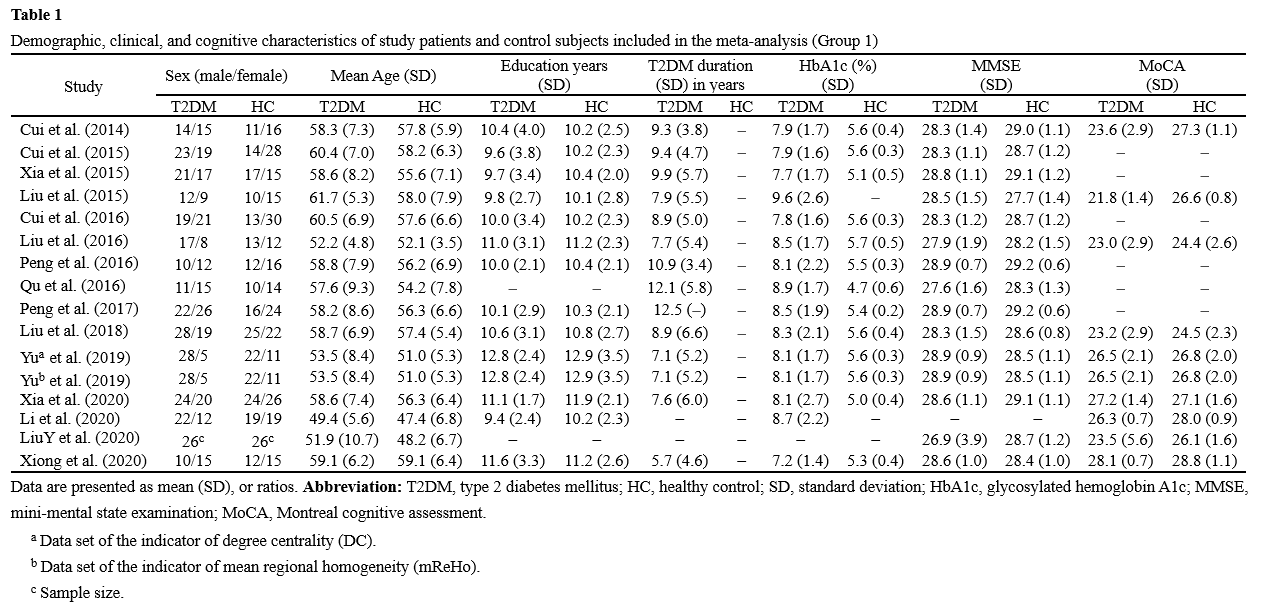
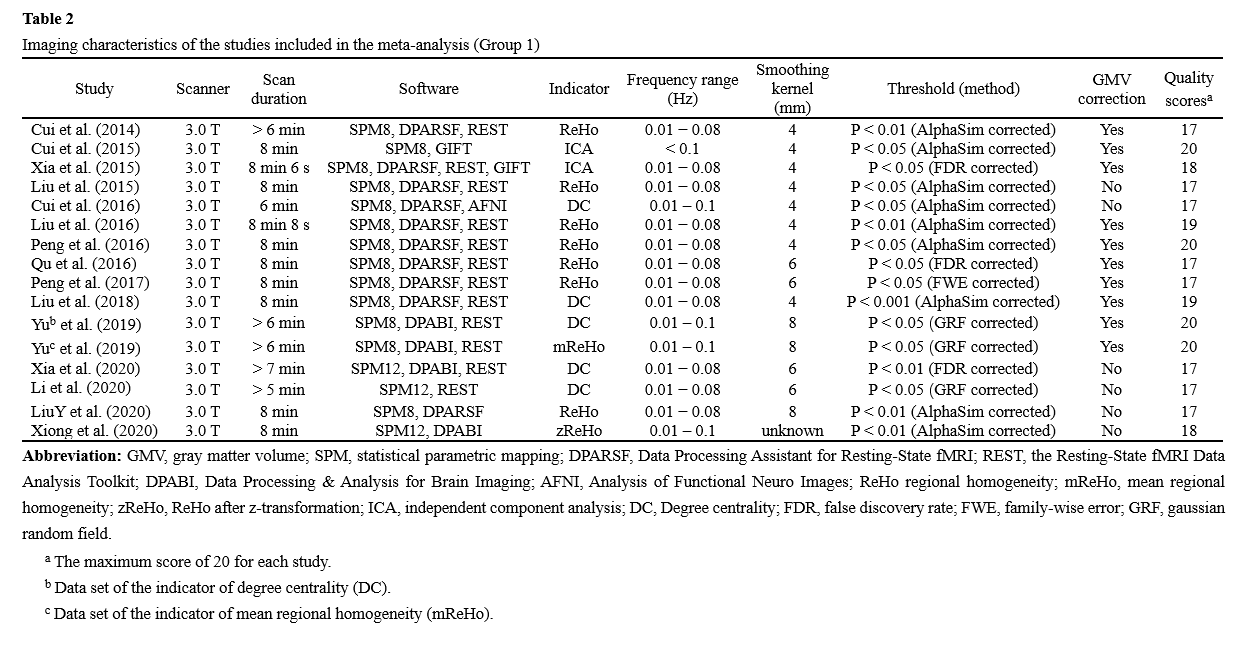
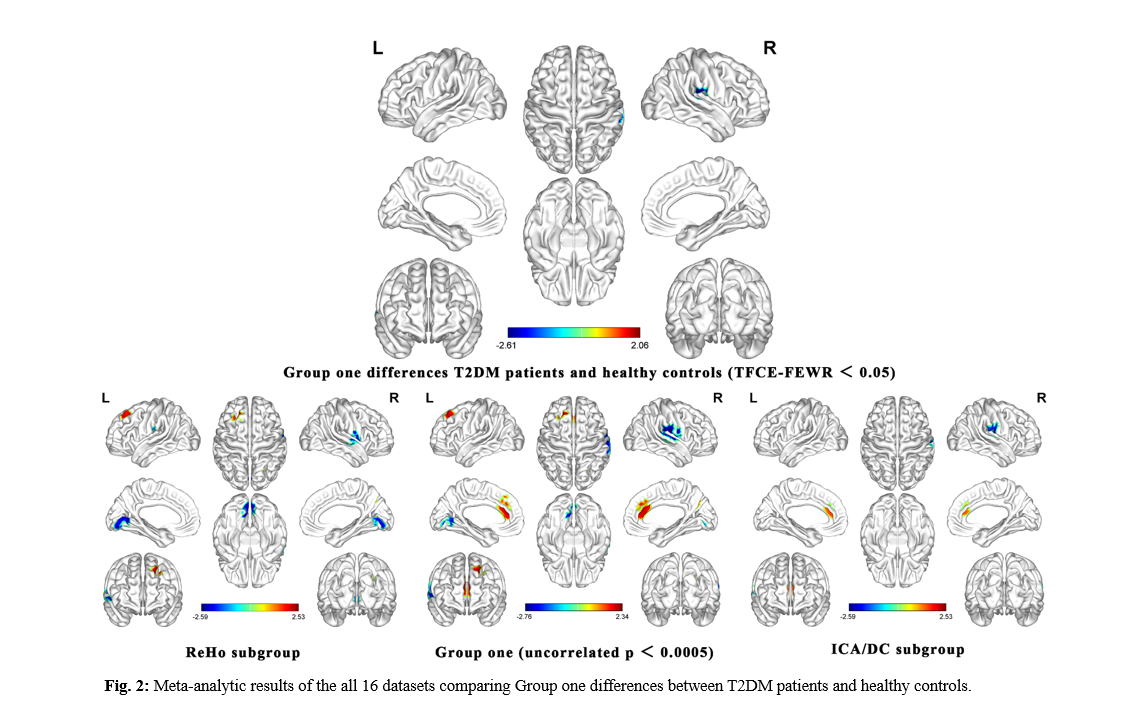
The final meta-analysis included 22 eligible trials with 26 data sets (Figure 1). The general information of the included literature is shown in Table 1 and Table 2. As shown in Figure 2, the group one of T2DM patients without MCI observed primarily in the right supramarginal gyrus, right postcentral gyrus, and right superior temporal gyrus as compared to healthy controls. In group two, there was no significant difference after correction. The results of PSI-SDM were summarized in Table 3.Conclusions
Our comprehensive meta-analysis showed that T2DM had a range of spontaneous abnormal brain activities, mainly involved in brain regions associated with learning, memory and emotion, which helped to understand the neuropathophysiological mechanism of T2DM. Although the results of single index meta-analysis may be more explanatory, the repeatability of the results of meta-analysis will be very low when there are less than 10 studies on the same indicator. Therefore, our team applied a strategy which divided the different functional imaging processing methods into two groups, including reflecting the intensity of neural activity in the brain and the relationship of neural activity in the brain. We found that the abnormal regions of different indexes have a certain consistency and high stability and repeatability. The main reason for the first group of heterogeneity was not caused by differences in indexes of brain function. Although ReHo, ICA and DC reflect the relationship of neural activity in the brain, their heterogeneity cannot be ignored. Therefore, we suggest that the results of a meta-analysis of a single index may be more explicable when ample studies are included. Conversely, when studies are scarce, we can divide the different functional imaging processing methods into reflecting-intensity and reflecting-relationship two groups, but we must carefully interpret the results. We believe this strategy is more reliable than a meta-analysis of all brain-function processing methods, but more in-depth research is needed.Acknowledgements
We thank each member of our team for their advice.References
References
1. Li Y, Teng D, Shi X, Qin G, Qin Y, Quan H, Shi B, Sun H, Ba J, Chen B, et al: Prevalence of diabetes recorded in mainland China using 2018 diagnostic criteria from the American Diabetes Association: national cross sectional study. Bmj 2020, 369:m997.
2. Li W, Sun L, Li G, Xiao S: Prevalence, Influence Factors and Cognitive Characteristics of Mild Cognitive Impairment in Type 2 Diabetes Mellitus. Front Aging Neurosci 2019, 11:180.
3. Sadanand S, Balachandar R, Bharath S: Memory and executive functions in persons with type 2 diabetes: a meta-analysis. Diabetes Metab Res Rev 2016, 32:132-142.
4. Farzi A, Hassan AM, Zenz G, Holzer P: Diabesity and mood disorders: Multiple links through the microbiota-gut-brain axis. Mol Aspects Med 2019, 66:80-93.
5. van Sloten TT, Sedaghat S, Carnethon MR, Launer LJ, Stehouwer CDA: Cerebral microvascular complications of type 2 diabetes: stroke, cognitive dysfunction, and depression. Lancet Diabetes Endocrinol 2020, 8:325-336.
6. Bellary S, Kyrou I, Brown JE, Bailey CJ: Type 2 diabetes mellitus in older adults: clinical considerations and management. Nat Rev Endocrinol 2021, 17:534-548.
7. Zang Y, Jiang T, Lu Y, He Y, Tian L: Regional homogeneity approach to fMRI data analysis. Neuroimage 2004, 22:394-400.
8. Hyvärinen A, Oja E: Independent component analysis: algorithms and applications. Neural Netw 2000, 13:411-430.
9. Yu Y, Yan LF, Sun Q, Hu B, Zhang J, Yang Y, Dai YJ, Cui WX, Xiu SJ, Hu YC, et al: Neurovascular decoupling in type 2 diabetes mellitus without mild cognitive impairment: Potential biomarker for early cognitive impairment. Neuroimage 2019, 200:644-658.
10. Zang YF, He Y, Zhu CZ, Cao QJ, Sui MQ, Liang M, Tian LX, Jiang TZ, Wang YF: Altered baseline brain activity in children with ADHD revealed by resting-state functional MRI. Brain Dev 2007, 29:83-91. 11. Alsop DC, Detre JA, Golay X, Günther M, Hendrikse J, Hernandez-Garcia L, Lu H, MacIntosh BJ, Parkes LM, Smits M, et al: Recommended implementation of arterial spin-labeled perfusion MRI for clinical applications: A consensus of the ISMRM perfusion study group and the European consortium for ASL in dementia. Magn Reson Med 2015, 73:102-116.
12. Müller VI, Cieslik EC, Laird AR, Fox PT, Radua J, Mataix-Cols D, Tench CR, Yarkoni T, Nichols TE, Turkeltaub PE, et al: Ten simple rules for neuroimaging meta-analysis. Neurosci Biobehav Rev 2018, 84:151-161.
13. Page MJ, McKenzie JE, Bossuyt PM, Boutron I, Hoffmann TC, Mulrow CD, Shamseer L, Tetzlaff JM, Akl EA, Brennan SE, et al: The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. Bmj 2021, 372:n71.
14. Pan P, Zhu L, Yu T, Shi H, Zhang B, Qin R, Zhu X, Qian L, Zhao H, Zhou H, Xu Y: Aberrant spontaneous low-frequency brain activity in amnestic mild cognitive impairment: A meta-analysis of resting-state fMRI studies. Ageing Res Rev 2017, 35:12-21.
15. Albajes-Eizagirre A, Solanes A, Vieta E, Radua J: Voxel-based meta-analysis via permutation of subject images (PSI): Theory and implementation for SDM. Neuroimage 2019, 186:174-184.
Figures