3040
Head and Neck DWI: Comparison of Image Quality and Diagnostic Performance among FASE and EPI Sequences with and without DLR1Radiology, Fujita Health University School of Medicine, Toyoake, Japan, 2Canon Medical Systems Corporation, Otawara, Japan, 3Joint Research Laboratory of Advanced Medical Imaging, Fujita Health University School of Medicine, Toyoake, Japan, 4Radiology, Fujita Health University Hospital, Toyoake, Japan
Synopsis
No major studies have been reported for assessing the utility of DWI obtained by Fast Advanced Spin-Echo (FASE) with Deep Learning Reconstruction (DLR) for head and neck MR. We hypothesized that DWI obtained by FASE with DLR could improve the image quality with less deformation and better diagnostic performance as compared with DWI obtained by Echo-Planar Imaging (EPI) in head and neck MR. The purpose of this study was to compare the capability of DWI obtained by FASE and EPI sequences with and without DLR for image quality and diagnostic performance on DWI in patients suspected head and neck tumors.
Introduction
Diffusion-weighted imaging (DWI) has been clinically applied and considered as one of the key sequences to differentiate malignant from benign lesions in head and neck MRI since 2000s. One of the problems for head and neck MRI is degradation of image quality, lesion conspicuity and influence to apparent diffusion coefficient (ADC) measurement because of susceptibility artifact from air-soft tissue interfaces at complicated structures in paranasal sinus, oral cavity, pharynx and larynx. Although echo-planar imaging (EPI) sequence is usually applied for head and neck DWI, major drawbacks are considered as low spatial resolution and severe distortion in routine clinical practice1. To overcome these drawbacks, fast advanced spin-echo (FASE) sequence has also been proposed as another sequence for DWI because FASE is more tolerance to susceptibility artifact in not only head and neck, but also thoracic MRI in the last decade2, 3. However, relatively low signal to noise ratio (SNR) has been considered as one of the problems on DWI obtained by FASE sequence2, 3. Deep learning reconstruction (DLR) has recently been introduced to improve image quality as one of the noise reduction methods in not only MRI, but also CT4, 5. However, no major studies have been reported for assessing the utility of DWI obtained by FASE with DLR for head and neck MR imaging. We hypothesized that DWI obtained by FASE with DLR could improve the image quality with less deformation and better diagnostic performance as compared with conventional DWI obtained by EPI in head and neck MR imaging. The purpose of this study was to compare the capability of DWI obtained by FASE and EPI sequences with and without DLR for image quality and diagnostic performance on DWI in patients suspected head and neck tumors.Methods
This study included with in vitro and in vivo studies.As first study, in vitro study was performed. A QIBA DWI phantom (128QIBA diffusion phantom: CaliberMRI, Boulder, Colorado, USA) was scanned at a 3T scanner (Vantage Centurian, Canon Medical Systems Corporation, Otawara, Japan) by DWIs with FASE and EPI sequences. Then, each data was reconstructed with and without DLR (Advanced intelligent Clear-IQ Engine [AiCE], Canon Medical Systems). Then, ADC within each phantom was measured. To determine the relationship between measured and actual ADC within each phantom, Pearson’s correlation was performed.
As second study, in vivo study was performed. 58 head and neck tumor patients who had 26 malignant and 32 benign lesions underwent T2WI and DWIs by FASE and EPI sequences. Then, each DWI was also reconstructed with and without DLR. SNR and ADC of each lesion were assessed by ROI measurements. To compare image deformation between all DWIs, the margin of lesion was traced by free hand ROI on each sequence to assess each lesion deformation. Then, deformation ratio (DR) was defined as free hand ROI area difference between each DWI and T2WI divided by ROI area on T2WI. To compare the difference of tumor DR at each location, the tumor locations were categorized into as follows: 1) pharynx and larynx, 2) oral cavity and mandibular, 3) salivary glands and 4) others. Then, DR and SNR were compared among all DWIs at each category by paired t-test. To determine feasible threshold values of each DWI for differentiation of malignant from benign lesions, ROC analysis was performed. Finally, sensitivity, specificity and accuracy were compared among all DWI methods by McNemar’s test.
Results
On in vitro study, there were significant and excellent correlations between measured and actual ADCs on DWIs obtained by FASE and EPI sequences and reconstructed with and without DLR (0.95<r<0.99, p<0.0001).On in vivo study, DRs of FASE with DLR were significantly smaller than those of EPI with and without DLR in 1) pharynx and larynx and 2) oral cavity and mandibular (p<0.05), whereas there were not significant difference of DR among all methods in 3) salivary glands and 4) others (p>0.05) (Figure 2). Compared SNR among all DWI methods are shown in Figure 3. SNR of FASE with DLR at each category was significantly higher than that without DLR (p<0.05). Moreover, SNR of EPI with DLR at 4) others category was significantly higher than that without DLR (p<0.05). ROC analysis results are shown in Figure 4. Feasible threshold value for each DWI was determined as follows: EPI without DLR; 1.316 x 10-3mm2/s, EPI with DLR; 1.376 x 10-3mm2/s, FASE without DLR; 1.491 x 10-3mm2/s, FASE with DLR; 1.412 x 10-3mm2/s. Comparison of diagnostic performance among all DWIs is shown in Figure 5. There were no significant differences of sensitivity, specificity and accuracy among all DWIs (p>0.05).
Conclusion
On head and neck DWI, FASE sequence has a potential for improving lesion deformation as compared with EPI sequence. Moreover, DLR is able to improve image quality on DWI, especially FASE sequence. Although diagnostic performance of ADC had no significant difference among all DWIs, this fact is compatible with our in vitro study results and easy to be speculated.Acknowledgements
This study was technically and financially supported by Canon Medical Systems Corporation.References
1. Verhappen M, Pouwels P, Ljumanovic R, et al. Diffusion-weighted MR imaging in head and neck cancer: comparison between half-fourier acquired single-shot turbo spin-echo and EPI techniques. Am J Neuroradiol. 2012 Aug;33(7):1239-46
2. Ohno Y, Koyama H, Yoshikawa T, et al. Diffusion-weighted MR imaging using FASE sequence for 3T MR system: Preliminary comparison of capability for N-stage assessment by means of diffusion-weighted MR imaging using EPI sequence, STIR FASE imaging and FDG PET/CT for non-small cell lung cancer patients. Eur J Radiol. 2015 Nov;84(11):2321-31.
3. Mikayama R, Yabuuchi H, Sonoda S, et al. Comparison of intravoxel incoherent motion diffusion-weighted imaging between turbo spin-echo and echo-planar imaging of the head and neck. Eur Radiol. 2018 Jan;28(1):316-324.
4. Matsukiyo R, Ohno Y, Matsuyama T, et al. Deep learning-based and hybrid-type iterative reconstructions for CT: comparison of capability for quantitative and qualitative image quality improvements and small vessel evaluation at dynamic CE-abdominal CT with ultra-high and standard resolutions. Jpn J Radiol. 2021 Feb;39(2):186-197.
5. Ueda T, Ohno Y, Ikeda H, et al. Compressed sensing and deep learning reconstruction for women's pelvic MRI denoising: Utility for improving image quality and examination time in routine clinical practice. Eur J Radiol. 2021 Jan;134:109430.
Figures
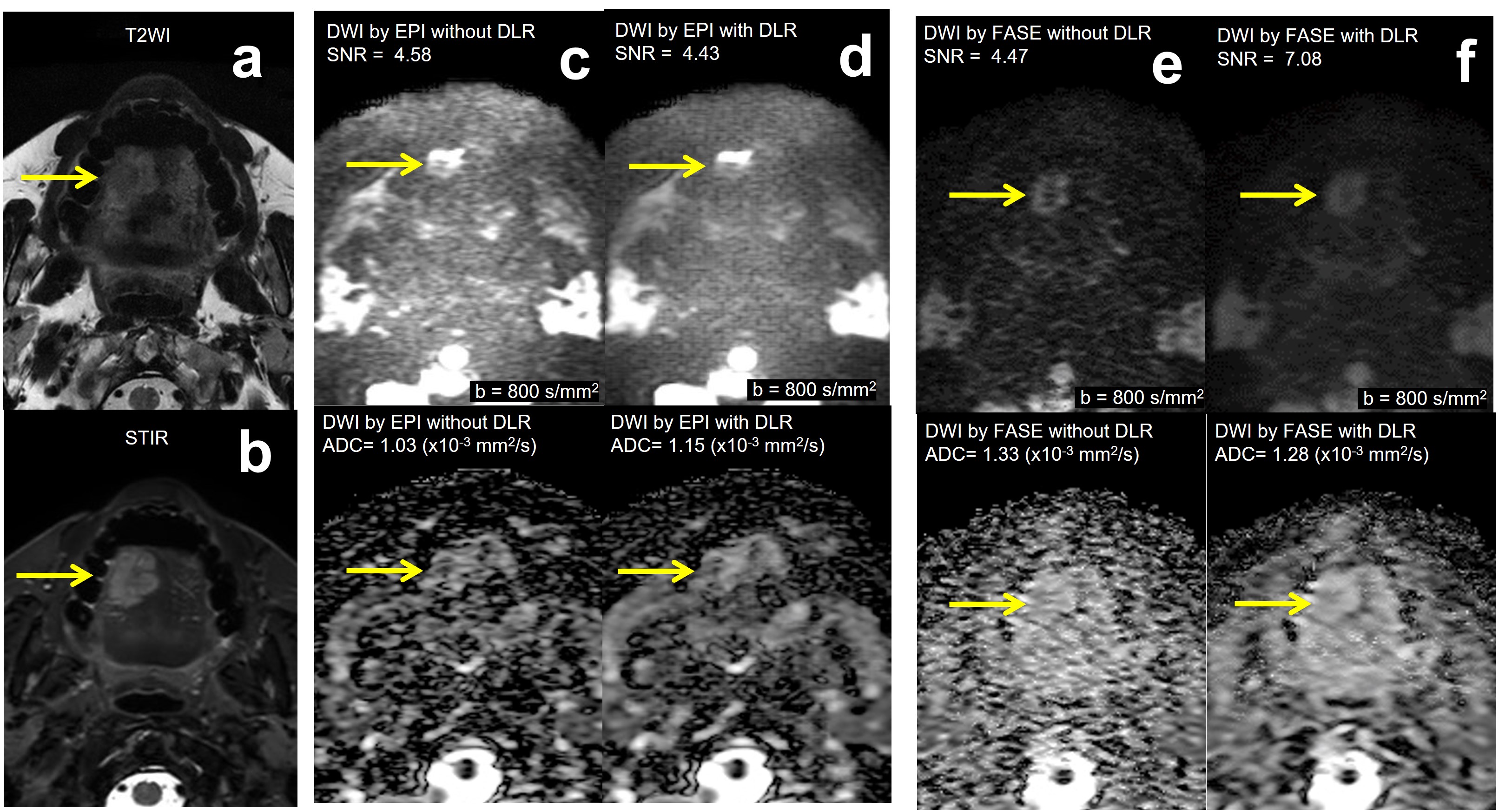
FIgure 1. 39 years old male with oral cavity cancer (T3N0M0).
Lobulated shape of tumor on right side of tongue is well depicted on T2WI and STIR (a, b). When compared with T2WI, the tumor on DWIs by EPI with and without DLR are deformed (c, d). The tumor on DWIs by FASE with and without DLR are less deformed and lobulated shape is preserved (e, f). SNR of DWI obtained by FASE with DLR was higher than that without DLR. There were no significant differences of ADC among all DWIs.
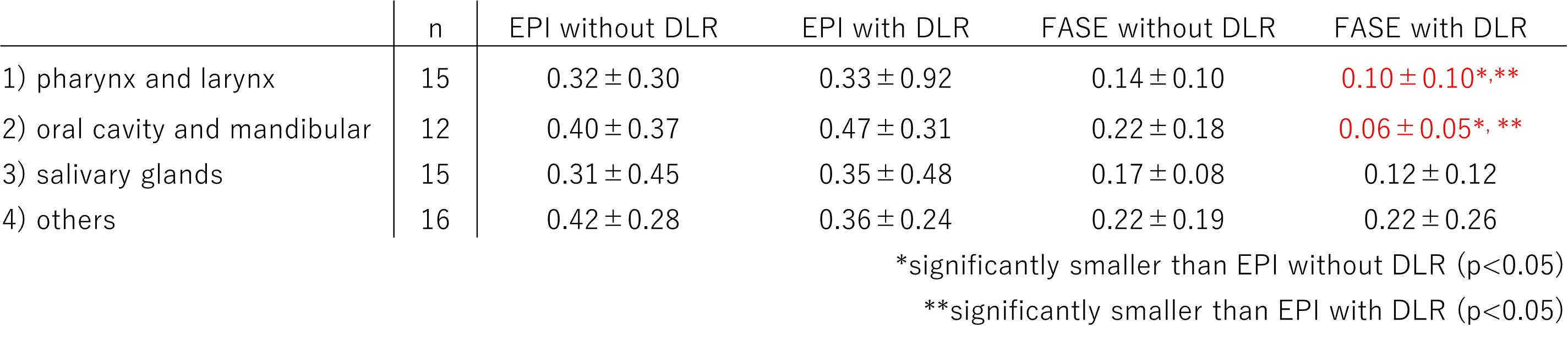
FIgure 2. Results of Comparison for DR (Deformation Ratio) of EPI and FASE with and without DLR in each location.
DR of FASE with DLR was significantly smaller than EPI with and without DLR in 1) pharynx and larynx and 2) oral cavity and mandibular (p<0.05).

FIgure 3. Result of comparison for SNR of each method with and without DLR in each location.
SNRs of FASE with DLR were better than FASE without DLR at each category (p<0.05), altough SNR of EPI with DLR was better than EPI without DLR at 4) ohters category (p<0.05).
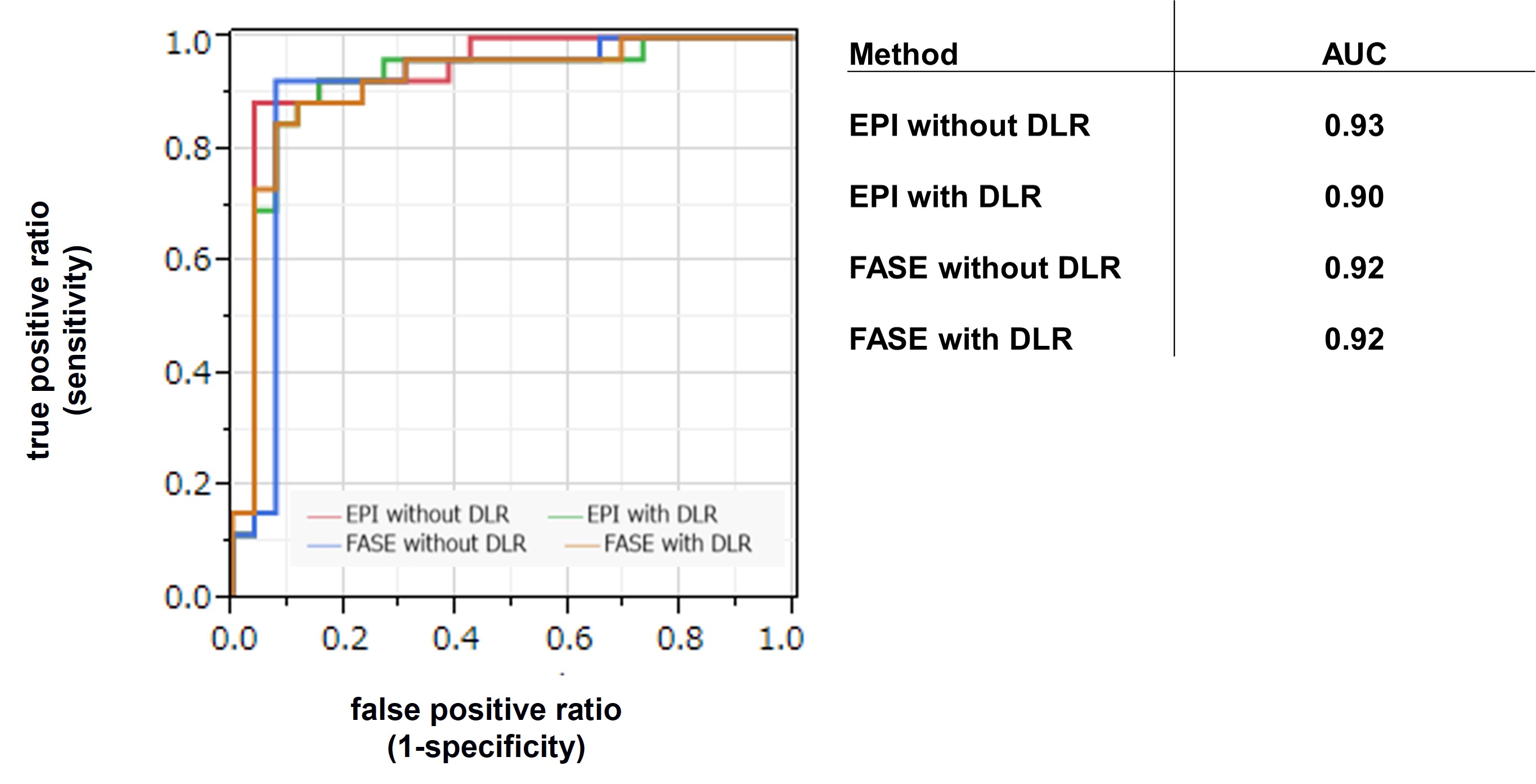
FIgure 4. Result of ROC analysis.
There were not significant differences of AUCs among all methods (p>0.05).
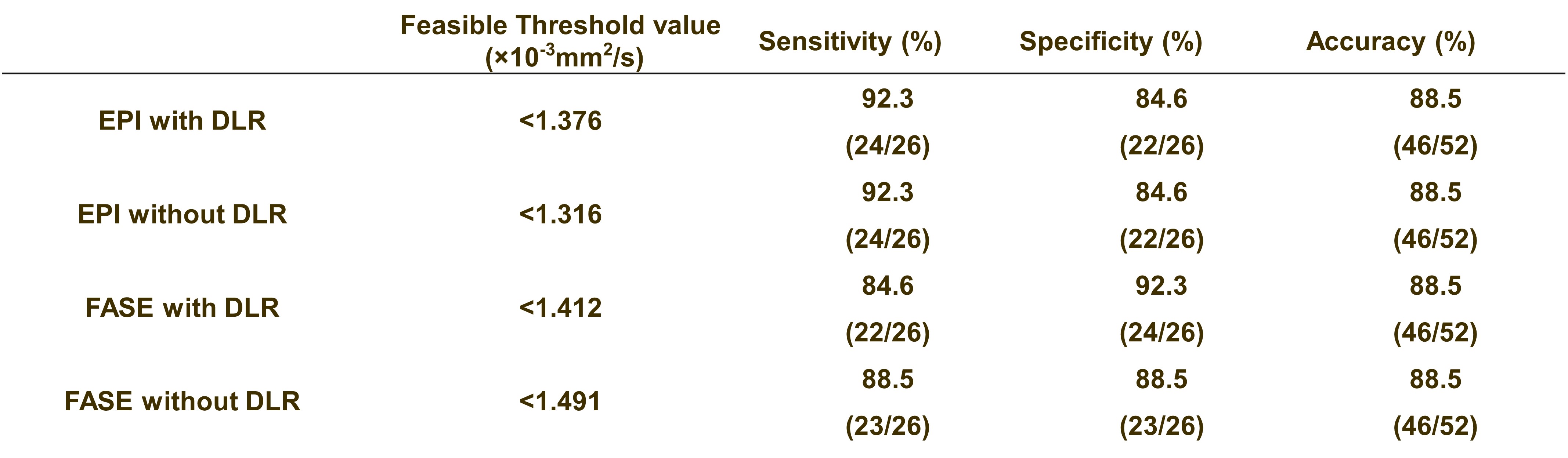
FIgure 5. Results of Comparison of diagnostic performance among EPI and FASE with and without DLR.
When applied each feasible threshold value, sensitivity, specificity and accuracy had no significant difference among all methods (p>0.05).