3022
3D T2-FFE MR Neurography of lumbosacral plexus with a deep learning constrained Compressed SENSE reconstruction1Radiology, First Hospital of Jilin University, changchun, China, 2Philips Heathcare, Beijing, China
Synopsis
Three-dimensional (3D) T2 Fast Field Echo (FFE) sequence of MR Neurography always takes a very long scan time. However, using very high acceleration factors (AF) will result in degradation of image quality due to insufficient noise removal. In this study, we used Compressed-SENSE Artificial Intelligence (CS-AI) framework to acquire highly accelerated T2 FFE imaging in lumbosacral plexus. The results showed that CS-AI reconstruction might significantly decrease scan time with sufficient image quality compared with conventional SENSE, and might be clinically useful for assessment of lumbosacral plexus.
Introduction
Three-dimensional (3D) imaging with T2 Fast Field Echo (FFE) sequence is thought to be of great capability to depict and evaluating lumbosacral plexus anatomy in the abdomen and pelvis 1-2. However, the approaches using such sequence still face some challenges due to its long scan time consumption and contamination by artifacts. Combined sensitivity encoding (SENSE) and compressed sensing (Compressed SENSE, CS) have been proven to achieve scan time reduction beyond that possible with conventional parallel imaging acceleration 3-4. However, using very high AF with very high resolution can result in degradation of image quality due to insufficient noise removal. More recently, deep learning-based algorithms have been combined with CS to overcome these challenges by learning optimal reconstruction parameters from the data itself and showed superior performance in knee MR image reconstruction from highly undersampled k-space data 5-8.Purpose
The purpose of this study was to acquire highly accelerated 3D T2 FFE imaging in lumbosacral plexus using the Compressed-SENSE Artificial Intelligence (CS-AI) framework reconstruction and to evaluate the image quality of CS-AI and CS with different AF compared with conventional SENSE parallel imaging technique.Methods
A total of 20 volunteers were examined on a 3.0 T MR system (Ingenia Elition X, Philips Healthcare), including 5 men and 15 women (mean age 47.85±17.3 years, range: 21-79 years). This study was approved by the local IRB, and written informed consent was obtained from all subjects. All subjects received different customized 3D T2 FFE sequences which included two different AF sequences utilizing CS-SENSE (CS 3, CS 6) and CS-AI technology (CS-AI 3, CS-AI 6), and 1 sequence utilizing traditional SENSE technology used as reference (SENSE factors 2). The following parameters were common to all examinations: voxel size =0.99*1.00*1.80 mm 3, FOV =270*214*90 mm, Slices=100, TR =8.0 ms, TE =4.0 ms, Flip angle=30°, TSE factor =40, NSA=2. The scan results were exported to Philips IntelliSpace Portal (ISP, Philips Healthcare). Quantitative image analysis was performed by a radiologist with more than 4 years of experience. Signal to noise ratio (SNR) and contrast to noise ratio (CNR) were calculated by setting the nerve root as the region of interest (ROI) and setting the psoas muscle as a contrast. The image quality of CS and CS-AI was visually compared, including anatomical structures, diagnostic certainty and artifacts scored with a five-point scale.The paired Wilcoxon test was performed to test for an influence of the different sequences. P values< 0.05 were considered significant.Results
Scan time decreased with increasing of AF (SENSE 3min31s, CS 3 1min22s, CS 6 42s). For quantitative analysis of image quality, the SNR values in all different AF sequences were not statistically significant compared with the reference SENSE sequence. With the increase of AF, the CNR values of CS 3, CS 6 and CS-AI 6 were all significantly lower than SENSE (P<0.05), but the CNR values was not statistically significant between CS-AI 3 and SENSE. On the other hands, the CNR value of CS-AI 6 and CS-AI 3 and the SNR value of CS-AI 3 were significantly higher than the CS sequences with the same AF ( P<0.05).For subjective analysis, the scores of all subject of CS 3, CS 6 and CS-AI 6 sequences were significantly lower than SENSE (p<0.05). CS-AI 3 clearly improved the scores of imaging artifacts with an average of 4.58±1.25 compared with SENSE (P<0.05) and showed equivalent delineation and clarity of anatomical structures and diagnostic certainty. With the increase of AF, all subjective scores decreased clearly (p <0.05). However, the scores of CS-AI 6 were significantly higher than CS 6 in terms of anatomical structures, diagnostic certainty and artifacts, and it was for artifacts also CS-AI 3 (p <0.05). The mean SNR, CNR and subject scores for all sequences were listed in the Table1. The representative high resolution T2 FFE images using the SENSE, CS and CS-AI reconstructions with different AF were shown in Figure 1 and Figure 2.Conclusion
CS-AI reconstruction can significantly decrease the scan time of 3D T2 FFE neurography in the lumbosacral plexus, with sufficient image quality compared with conventional SENSE. CS-AI 3 even provided better image quality while reducing scan time (61.14%). Although further clinical investigation is needed, high-resolution T2 FFE with CS-AI reconstruction might be clinically useful for assessment of lumbosacral plexus.Acknowledgements
No acknowledgement found.References
1.Chhabra A, Rozen S, Scott K. Three-dimensional MR neurography of the lumbosacral plexus. Semin Musculoskelet Radiol 2015; 19(2): 149-59.
2.Kim SW, Kim CH, Kim MS, Jung YJ, Byun WM. Usefulness of Three Dimensional Proset MR Images for Diagnosis of Symptomatic L5-S1 Foraminal and Extraforaminal Stenosis. J Korean Neurosurg Soc 2013; 54(1): 30-3.
3.Bratke G, Rau R, Kabbasch C, et al. Speeding up the clinical routine: Compressed sensing for 2D imaging of lumbar spine disc herniation. Eur J Radiol 2021; 140: 109738.
4.Iuga AI, Abdullayev N, Weiss K, et al. Accelerated MRI of the knee. Quality and efficiency of compressed sensing. Eur J Radiol 2020; 132: 109273.
5.Knoll F, Zbontar J, Sriram A, et al. fastMRI: A Publicly Available Raw k-Space and DICOM Dataset of Knee Images for Accelerated MR Image Reconstruction Using Machine Learning. Radiol Artif Intell. 2020;2(1):e190007.
6.Knoll F, Murrell T, Sriram A, et al. Advancing machine learning for MR image reconstruction with an open competition: Overview of the 2019 fastMRI challenge. Magn Reson Med. 2020;(January):mrm.28338.
7.Pezzotti N, Yousefi S, Elmahdy MS, et al. An Adaptive Intelligence Algorithm for Undersampled Knee MRI Reconstruction. IEEE Access. 2020;8:204825-204838.
8.Pezzotti N, de Weerdt E,Yousefi S, et al. Adaptive-CS-Net: FastMRI with Adaptive Intelligence. arxiv. 2019;(NeurIPS).
Figures
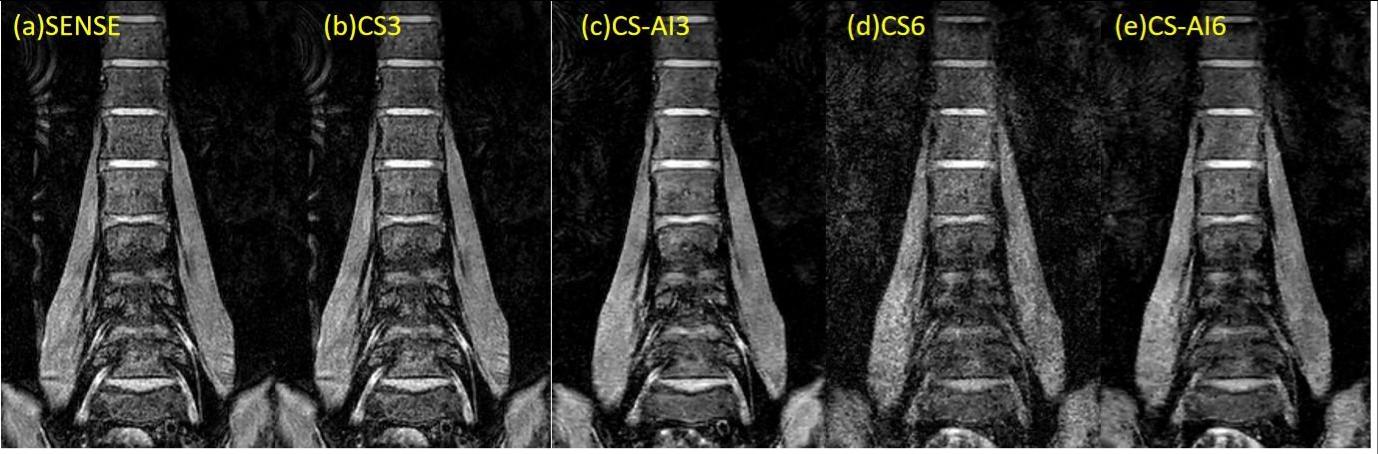

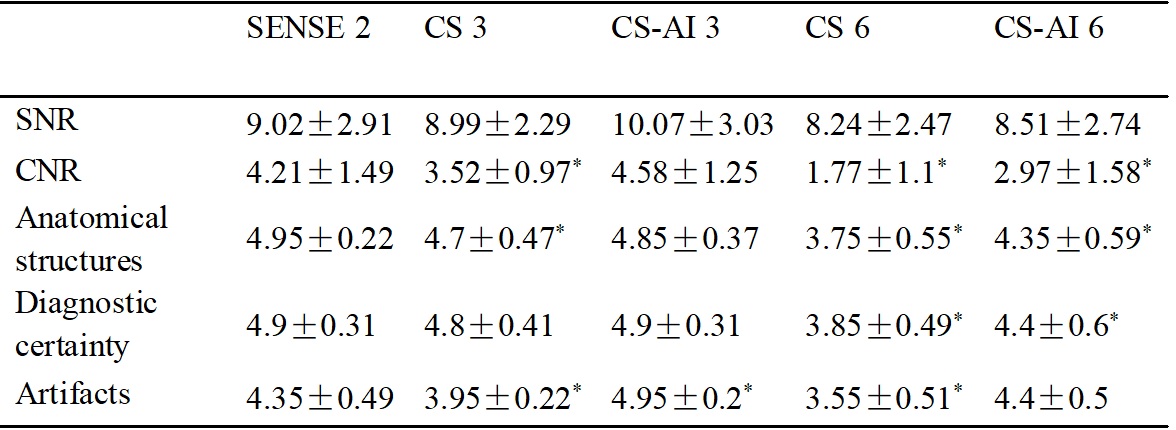
Table 1
* denotes statistically significant differences (p < 0.05) compared to the SENSE sequences.