3019
Pudendal nerve involvement in young men with erectile dysfunction: demonstration by 3T MR neurography1Departments of Radiology, Shandong Provincial Hospital Affiliated to Shandong First Medical University, Jinan, Shandong, 250021, China, Jinan, China, 2Departments of Radiology, Shandong Provincial Hospital, Cheeloo College of Medicine, Shandong University, Jinan, Shandong, 250021, China, Jinan, China, 3Department of Radiology, Wuhu City Second People's Hospital, No. 259 Jiuhua Rd, Wuhu, 241000, Anhui, China., Wuhu, China, 4MSC Clinical & Technical Solutions, Philips Healthcare, Beijing, China., Beijing, China
Synopsis
More evidences have been identified that pudendal nerve was involved in the pathogenesis of erectile dysfunction (ED) in young men. This prospective study aimed to detect and quantify pudendal nerve alterations in young men with ED using 3T MR neurography protocol. Results certified that pudendal nerve could be visualized and quantified. T2 signal contrast ratio and nerve diameter of pudendal nerve were increased significantly in ED patients compared with healthy controls, suggesting the involvement of pudendal nerve in young men with ED and thus offering a new insight into the pathophysiology and treatment of ED.
Introduction
Erectile dysfunction (ED) is a major health problem worldwide that reduces the quality of life in men; the prevalence of ED is increasing in young men (younger than 40 years), estimated to be as high as 30% now. ED in young men was once thought to be entirely psychogenic, however, in the last few decades, the increasing attention has been attracted on organic etiology1. More evidences2 suggested that the involvement of the pudendal nerve was one of the primary causes of ED. This study aimed to assess the potential clinical utility of 3T magnetic resonance neurography (MRN) in pudendal nerve imaging using DWIBS and 3D NerveVIEW, and to detect and quantify pudendal nerve alterations in young men with ED.Methods
This prospective study was approved by the institutional ethics committee, and written informed consent was obtained from all participants. Totally 18 young men (age 35 ± 6 years) with ED and 20 age-matched healthy men were enrolled prospectively in this study, the scanning sequences including conventional pelvic MRI and high-resolution MRN. All participants underwent MRI examination on a 3.0 Tesla scanner (Achieva, Philips Healthcare, Best, The Netherlands) equipped with the dual-source parallel radio-frequency excitation and transmission technology. The 3D NerveVIEW sequence for MRN included the 3D high resolution T2-weighted turbo spin echo acquisition, the improved motion-sensitized driven equilibrium (iMSDE) module for reduced intra-lumen signal of veins, and accurate frequency inversion recovery (SPAIR) fat suppression. Parameters for 3D NerveVIEW were as follows: iMSDE preset pulse duration, 50 ms; SPAIR fat suppression; slice orientation, coronal; slice number, 190; and voxel size, 1.0 × 1.0 × 1.5 mm3. Parameters for DWIBS were as follows: single-shot EPI acquisition with double b-factors (0, 800 s/mm2); TR, 4034ms; TE, 73ms; slice number, 60; slice gap = 0 mm; inversion time, 260ms; EPI factor, 37; SENSE factor, 2.Two radiologists reconstructed blindly pudendal nerve (PN) using multi-planar reconstruction (MPR) and curved planar reconstruction (CPR) in 3D MRN, evaluated the visualization scores, and recorded T2 signal contrast ratio (CR) and diameter values of PN. The visualization score of PN was independently evaluated by the two observors using a 4-point scale: 4, excellent (these nerves were completely and clearly visualized with an excellent signal intensity); 3, good (these nerves were visualized and had a blurred edge and good signal intensity); 2, moderate (a part of PN and its main branches were visualized and were of moderate signal intensity); 1, poor (PN and its main branches were not visualized). The T2 CR (defined as T2 signal intensity of PN/adjacent obturator internus) and diameter values were measured at proximal, middle and distal segments of PN. The visualization scores of PN by the two observors were assessed by interclass correlation coefficient (ICC) analysis. Student’s t-test was used to compare the CR and diameter values of PN between ED patients and healthy controls. To determine the sensitivity and specificity of the CR and diameter values for discriminating differences between ED and HC, receiver operating characteristic (ROC) analyses was performed. P<0.05 was considered statistically significant. Statistical analysis was performed with the SPSS statistical software package (version 19.0; SPSS, IL, USA).
Results
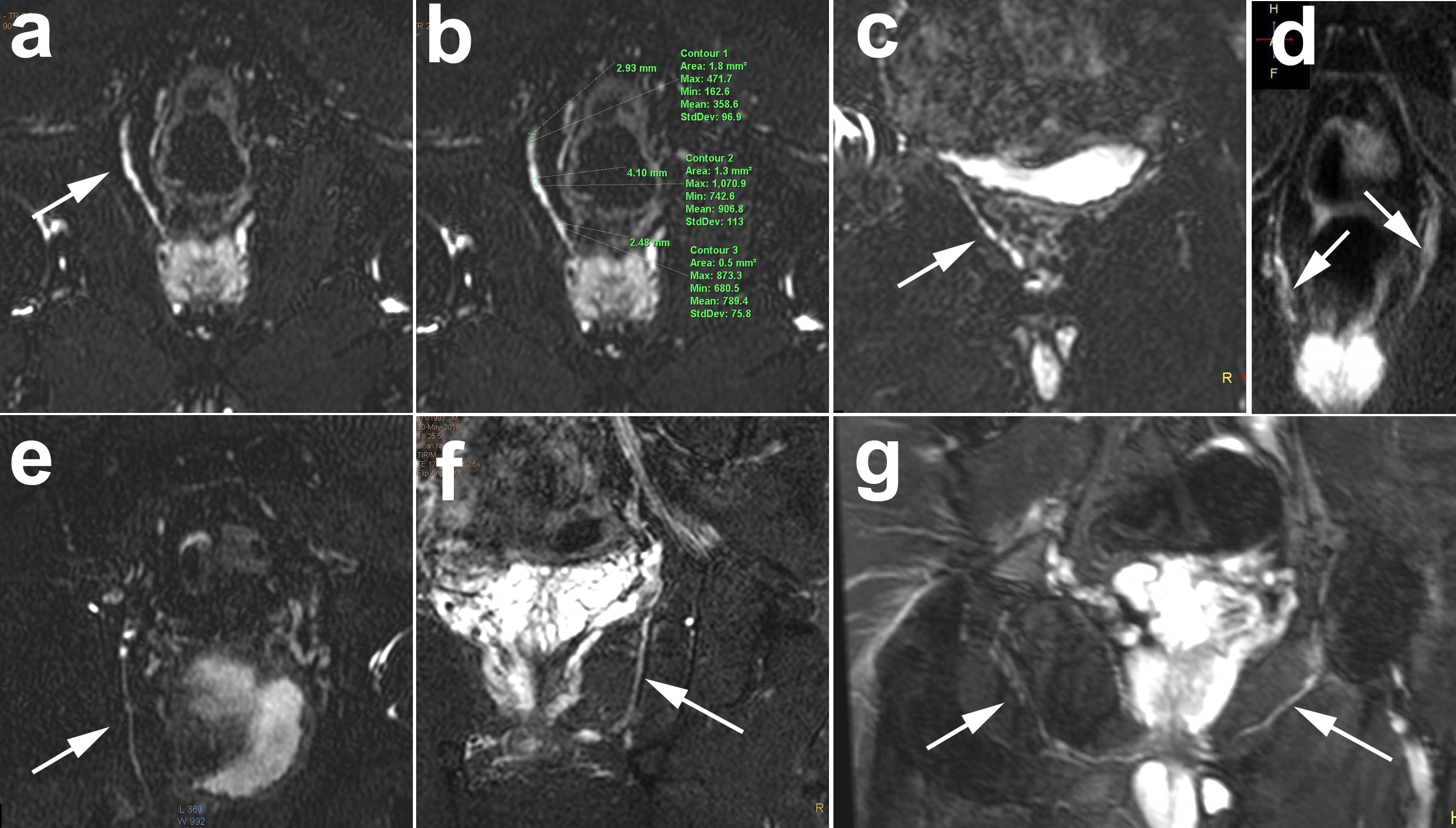
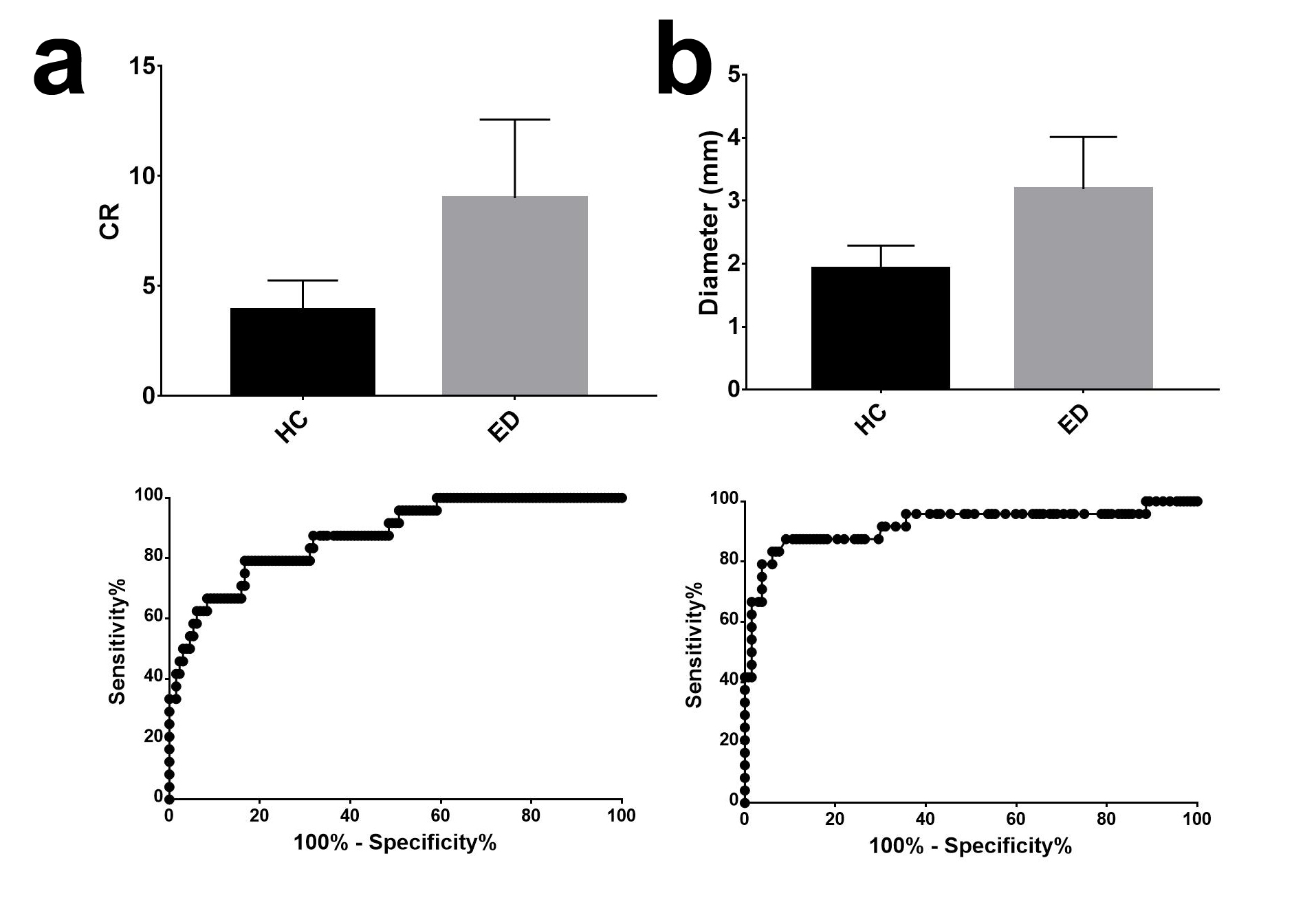
Pudendal nerve could be visualized well using MRN imaging, as shown in figure 1. The ICC for intra-reader agreement of visualization scores of PN in healthy volunteers and ED patients using 3T MRN were 0.880 [95% confidence interval (CI), 0.832–0.915] and 0.907 [95% CI, 0.743–0.966], respectively. T2 CR and diameter values of PN increased significantly in young men with ED compared with healthy controls (all p < 0.01). The ROC results showed that the CR value (AUC 87.37%, 95% CI 79.76% to 94.99%) and diameter value (AUC 92.12%, 95% CI 84.34% to 99.91%) had relatively high power to discriminate the ED patients, as shown in figure 2.Discussion
Results of this study certified that pudendal nerve could be visualized and quantified in young men using the thick-slab MPR and CPR images from 3D NerveVIEW. To our knowledge, this is the first time to confirm that T2 CR and diameter of PN were increased significantly in ED patients. The ROC results further found that CR and diameter value of PN were able to distinguish between young men with and without ED, suggesting that pudendal nerve was involved in the pathogenesis of ED. Our results was a strong evidence to support the prevailing clinical notion that pudendal nerve entrapment or compression may be a primary cause of ED3,4. A recent pilot study5 verified that surgical techniques for releasing the pudendal nerve could improve ED, suggesting some ED in young men was reversible, so the accurate etiological diagnosis is of utmost importance for the management of young men with ED.Conclusion
Pudendal nerve could be visualized and quantified in young men using 3T MRN. Increases in T2 signal contrast ratio and nerve diameter were shown in ED patients, suggesting the involvement of pudendal nerve in young men with ED and further offering a new insight into the pathophysiology and treatment of ED.Acknowledgements
This study was financially supported by Natural Science Foundation of Shandong (Grant No. ZR2020QH267)References
1. W L, M P. Organic causes of erectile dysfunction in men under 40. Urologia internationalis. 2014;92(1). doi:10.1159/000354931
2. Aoun F, Alkassis M, Tayeh GA, et al. Sexual dysfunction due to pudendal neuralgia: a systematic review. Transl Androl Urol. 2021;10(6):2500-2511. doi:10.21037/tau-21-13
3. Balasubramanian A, Yu J, Breyer BN, Minkow R, Eisenberg ML. The Association Between Pelvic Discomfort and Erectile Dysfunction in Adult Male Bicyclists. J Sex Med. 2020;17(5):919-929. doi:10.1016/j.jsxm.2020.01.022
4. Luther RD, Castellanos ME. Successful Treatment of Penile Numbness and Erectile Dysfunction Resulting From Pudendal Nerve Entrapment. Urology. 2019;134:228-231. doi:10.1016/j.urology.2019.09.010
5. Aoun F, Mjaess G, Daher K, et al. Laparoscopic treatment of pudendal nerve and artery entrapment improves erectile dysfunction in healthy young males. Int J Impot Res. 2021;33(1):1-5. doi:10.1038/s41443-020-0287-8
Figures