2978
Quantitative Evaluation of Spinal Cord Cine-MRI with Optical Flow Analysis1Department of Radiology, Tokai University Hospital, Isehara, Japan, 2Department of Health Sciences, Faculty of Medical Sciences, Kyushu University, Fukuoka, Japan, 3Philips Japan, Shinagawa, Japan, 4Department of Neurosurgery, Tokai University School of Medicine, Isehara, Japan, 5Department of Radiology, Tokai University School of Medicine, Isehara, Japan, 66) Department of Human and Information Science, School of Information Science and Technology, Tokai University, Hiratsuka, Japan
Synopsis
There are still many unclear issues in the motions of the spinal cord. This study is the first report to use optical flow analysis for quantitative evaluation of spinal cord motions. In the study of healthy volunteers, we found large displacement of the upper thoracic spinal cord. The study of clinical cases revealed that the spinal cord displacement changed before and after surgery. Therefore, these results suggested that quantitative evaluation of spinal cord motions is feasible using optical flow analysis.
Introduction
Spinal cord motions have been studied by MRI1,2. However, due to differences in imaging methods and measurement techniques, the precise motions of the spinal cord remain unclear. On the other hand, a detailed understanding of spinal cord motions is expected to improve image quality in DTI, MRS, etc. 3,4, and reduce the dose to the spinal cord in radiotherapy 5. Therefore, in this study, we attempted to quantitatively evaluate spinal cord motions using optical flow analysis on spinal cord cine-MRI. The purpose of this study was to evaluate the feasibility of quantitative evaluation of spinal cord motions using optical flow analysis in healthy volunteers and clinical cases.Material and Methods
This study protocol was approved by the Institutional Review Board of Tokai University Hospital. All of the volunteers and the patient were examined after obtaining appropriate written informed consent, consistent with the terms of our Institutional Review Board’s approval form. The subjects were 11 healthy volunteers (22-48 years old, 6 males and 5 females) and 2 clinical cases (cervical spondylosis: n = 1, Chiari malformation type I: n = 1). All examinations were performed on a 1.5 T scanner (Ingenia R5.3.1; Philips Healthcare, Best, the Netherlands). This system can operate at a maximum slew rate of 160 mT/m/ms and a maximum gradient strength of 66 mT/m. A 15-channel receive-only ds-Head Spine coil was used, covering the upper cerebellum to the upper thoracic spinal cord (Th 4). The basic parameters for electrocardiogram gated cine MRI were as follows: 2D balanced TFE, field of view: 250mm, voxel size: 1.0×0.95×5 mm, TR/TE: 4.3/2.1 ms, flip angle of 70°, reduction factor: 2 (phase), number of scan average :1, heart phase: 32, and scan time: 56 s. Optical flow analysis (MATLAB R2015a) was performed on the obtained Cine-MRI to measure the displacement of the spinal cord, medulla oblongata, and cerebellar tonsils. In healthy volunteers, the correlation between the displacement of spinal cord and height, heart rate, and cervical kyphosis angle was also examined. The theory of optical flow analysis is shown in Figure 1. The Mann-Whitney U test (MedCalc version 12.2.1) was used for statistical analysis.Result
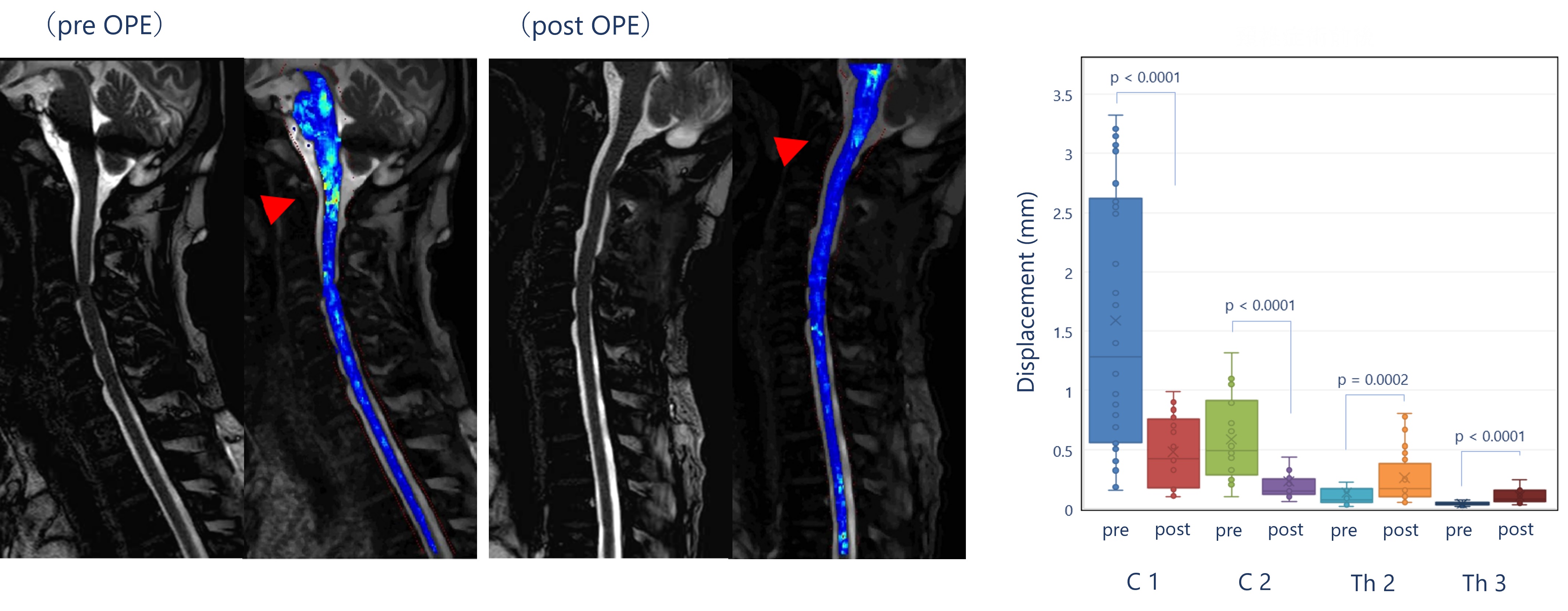
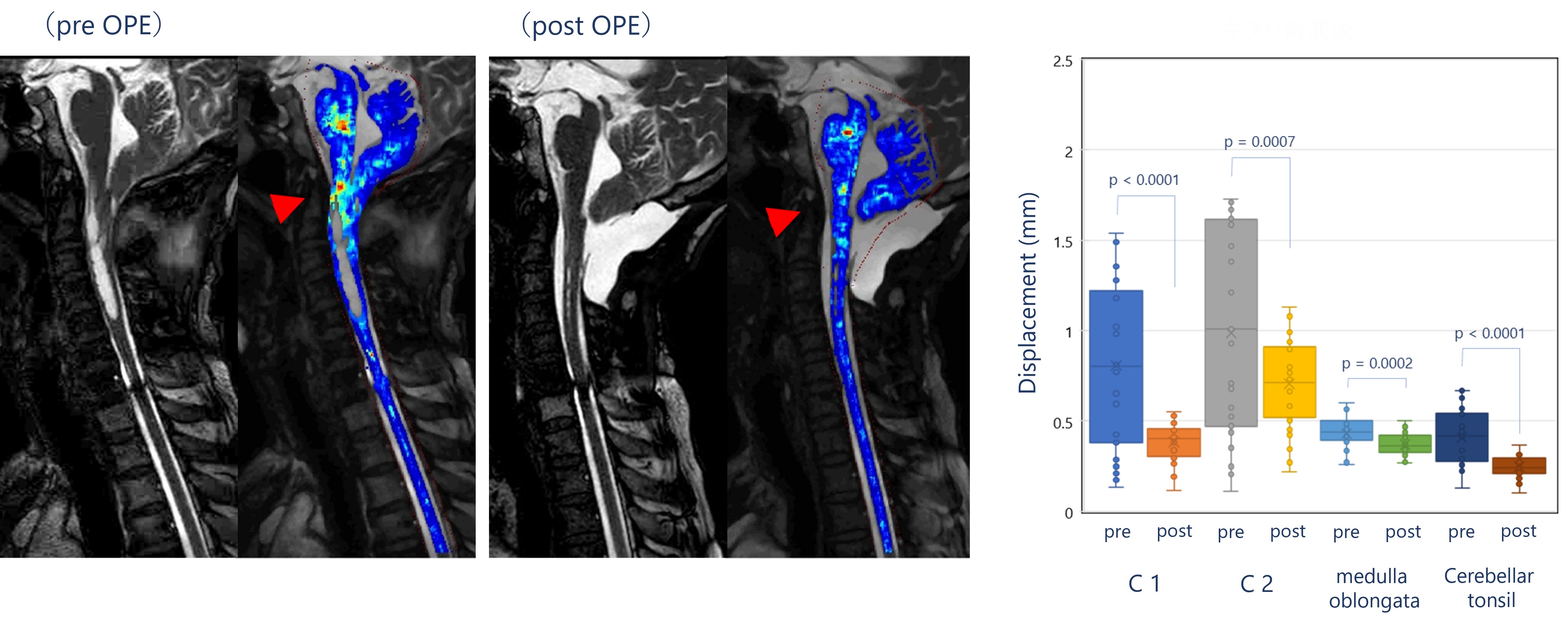
In healthy volunteers, the upper thoracic spinal cord (Th 2, 3) moved more than the cervical spinal cord in 73% (8/11) of cases. In addition, this displacement was greater during systole and was more pronounced in the anterior-posterior direction (Figure 2). However, this displacement was not correlated with height, heart rate, or cervical kyphosis angle. In clinical cases, significant changes in spinal cord motions were observed before and after surgery. In a cervical spondylosis case, the displacement in the cervical spinal cord above the stenosis (C3/4) was clearly reduced from preoperative (C1: 1.59 ± 1.09 mm, C2: 0.59 ± 0.33 mm) to postoperative (C1: 0.48 ± 0.31mm, C2: 0.23 ± 0.19 mm) (p<0.001, Figure 3). The displacement of the upper cervical spinal cord, medulla oblongata, and cerebellar tonsils was also reduced in a case with Chiari malformation type I after surgery (p<0.001, Figure 4).Discussion
This is the first report to use optical flow analysis for quantitative evaluation of spinal cord motions. In this study, we found that spinal cord motions can be quantitatively evaluated using optical flow analysis. In healthy volunteers, the upper thoracic spinal cord has greater displacement, which is consistent with previous studies. However, this displacement does not correlate with height or heart rate, which is inconsistent with previous studies. In the cervical spondylosis case, the stenosis caused excessive displacement in the medulla oblongata and upper cervical spinal cord, which was improved to normal displacement after the surgery. In Chiari malformation type I case, there was excessive displacement of the cerebellar tonsils before the surgery, which was reflected in the return to normal displacement after the surgery.Conclusion
The use of optical flow analysis on spinal cord Cine-MRI suggested that it is possible to quantitatively evaluate spinal cord motions.Acknowledgements
No acknowledgement found.References
1. Hupp M, Vallotton K, Brockmann C. et al. Segmental differences of cervical spinal cord motion: advancing from confounders to a diagnostic tool. Sci Rep. 2019 May 15;9(1):7415.
2. Winklhofer S, Schoth F, Stolzmann P. et al. Spinal cord motion: influence of respiration and cardiac cycle. Rofo. 2014 Nov;186(11):1016-21.
3. Summers P, Staempfli P, Jaermann T. et al. A preliminary study of the effects of trigger timing on diffusion tensor imaging of the human spinal cord. AJNR Am J Neuroradiol. 2006 Oct;27(9):1952-61.
4. Figley CR, Yau D, Stroman PW. Attenuation of lower-thoracic, lumbar, and sacral spinal cord motion: implications for imaging human spinal cord structure and function. AJNR Am J Neuroradiol. 2008 Sep;29(8):1450-4.
5. Oztek MA, Mayr NA, Mossa-Basha M. et al. The Dancing Cord: Inherent Spinal Cord Motion and Its Effect on Cord Dose in Spine Stereotactic Body Radiation Therapy. Neurosurgery. 2020 Jun 4;87(6):1157-1166.
Figures
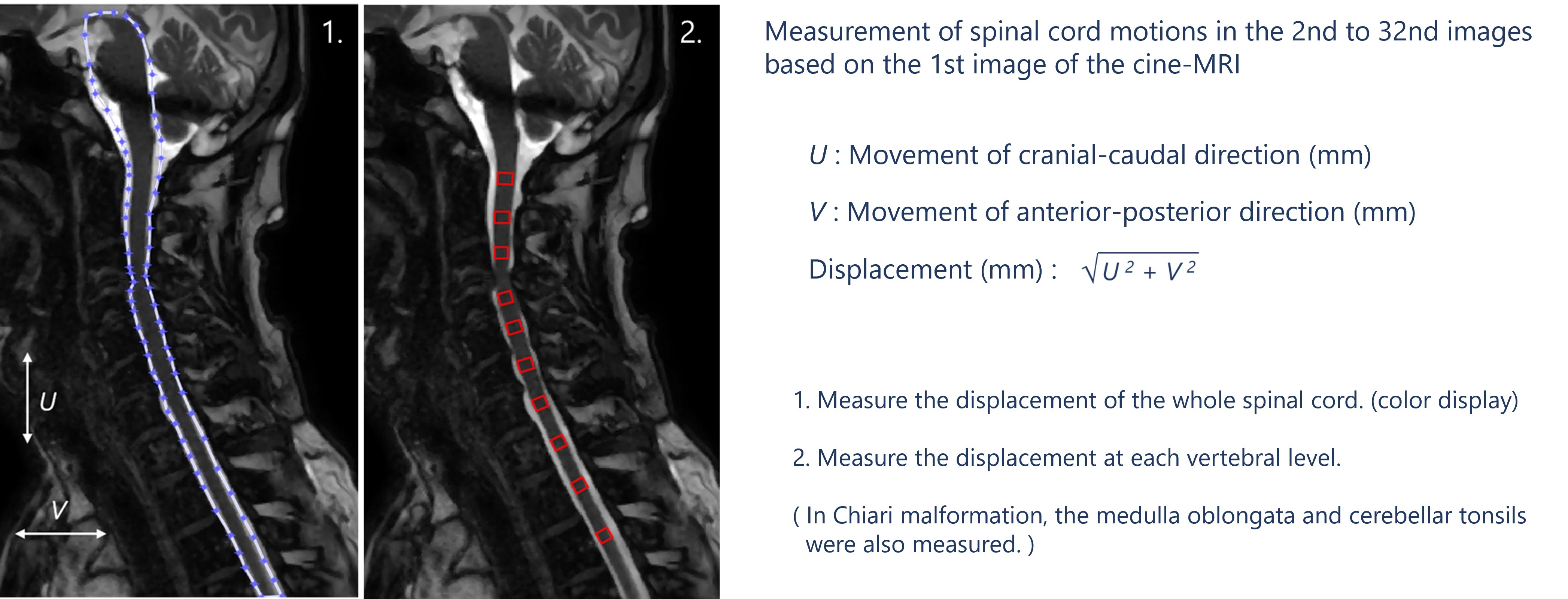
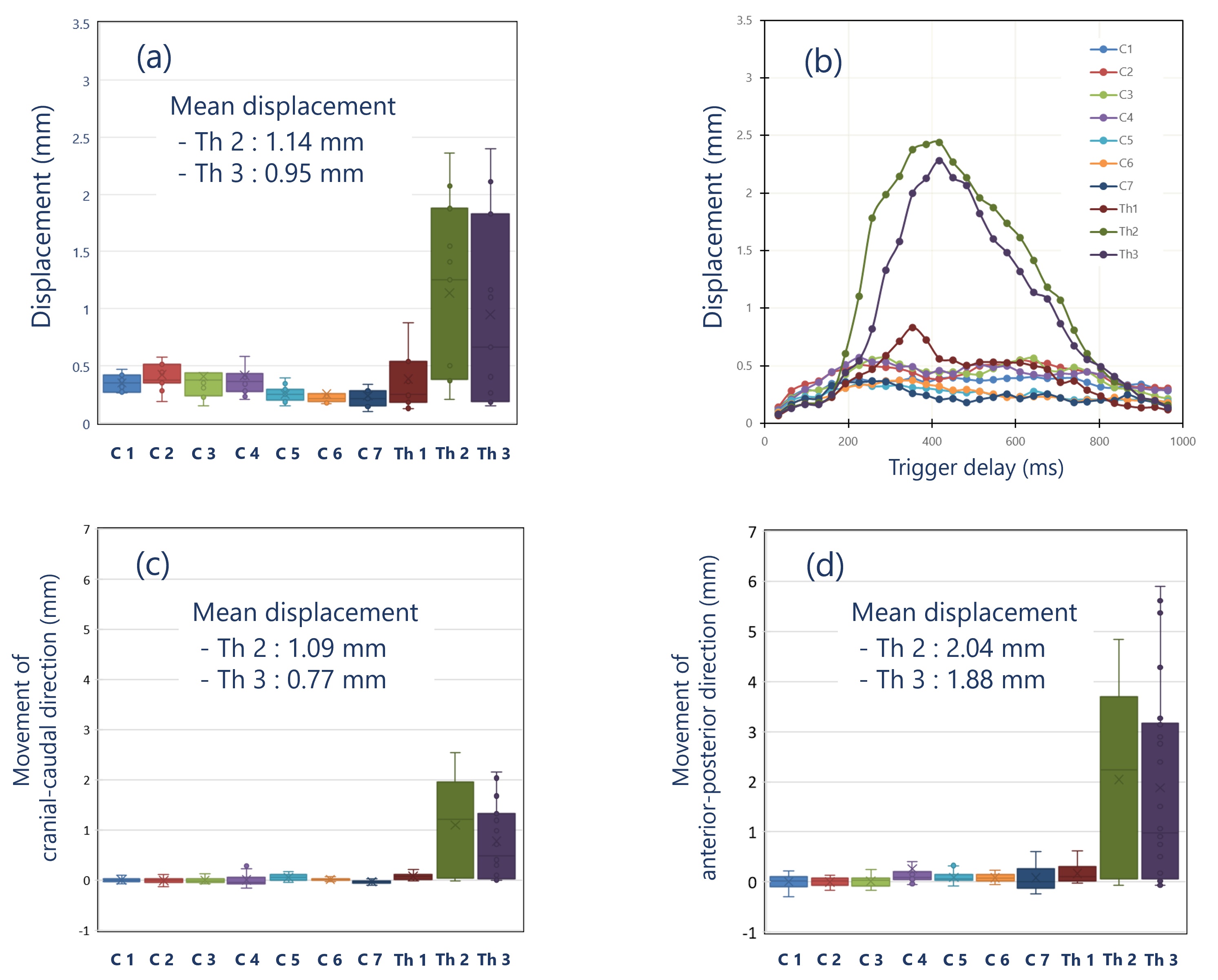
Figure 2. Displacement of the spinal cord in healthy volunteers. (a) Displacement of the spinal cord in healthy volunteers. (b) Displacement of the spinal cord during the cardiac cycle in healthy volunteers. (c) Movement of cranial-caudal direction. (d) Movement of anterior-posterior direction.