2948
A preliminary study of hemodynamic assessments of cerebral venous sinus stenosis using 4D flow MRI1the First Hospital of Jilin University, Chang Chun, China, 2MR Scientific Marketing, Siemens Healthineers, Bei Jing, China, 3MR Clinical Marketing, Siemens Healthineers Ltd, Bei Jing, China
Synopsis
4D flow MRI provides detailed insight into the alterations of hemodynamic,including quantitative assessment of flow parameters for the venous system. This technique overcomes the missing hemodynamic information of standard magnetic resonance imaging and the invasive disadvantage of digital subtraction angiography (DSA). Through data visualization and quantification, the particle tracking map is obtained and the peak velocities, wall shear stress (WSS) is calculated. The dynamics of venous sinus stenosis will change especially in severe area.
Introduction
Abnormal blood flow in the venous system can lead to a variety of cerebrovascular diseases. 4D flow MRI (time-resolved 3D phase-contrast MR imaging with 3-directional velocity-encoding) can be used to measure 3D cerebrovascular blood flow dynamics. Venous sinus stenosis which due to the cerebral venous thrombosis (CVT), idiopathic intracranial hypertension (IIH) and extrinsic compression can be evaluated. In this study, we aimed to demonstrate 4D flow MRI to investigate pathological intracerebral venous flow conditions in detail.Method
This study included six patients with venous sinus stenosis. Four acute extensive cerebral venous thrombosis patients could not be included because of the occluded vessel segments. Two cases with imaging characteristics on 4D flow MRI was invstigated in this study. 4D flow MR imaging was performed on a 3T system (MAGNETOM Vida, Siemens Healthcare, Erlangen, Germany) by using electrocardiographic gated. The following parameters were used: repetition time (TR) = 50.08; echo time (TE) = 3.66; slice thickness = 1.6mm; flip angle = 7°; VENC = 80cm/s. Total acquisition times for 4D flow MR imaging were dependent the heart rate and ranged between 15–20 minutes. In addition, magnetic resonance venography (MRV) scan was included in this study. Two radiologists evaluated all images using commercial software cvi 42, v.5.3 (Circle Cardiovascular Imaging, Calgary, Canada). Some preprocessing steps were performed before data visualization and quantification, such as eddy current correction, velocity aliasing correction and vessel segmentation. The cross-sections were inserted in the stenosis and the proximal and distal ends of the stenosis. For quantification of blood flow, cross-sections were perpendicular to the vessels of interest. For each analysis plane, peak velocities (m/s),WSS (Pa) and lumen area at maximum stenosis(mm2)were calculated in a cardiac cycle by the software. The blood flow distribution characteristics of intracranial venous system were analyzed according to particle tracking map.Result
The results of this study demonstrate the potential of 4D flow MRI for the comprehensive evaluation of hemodynamics in patients with venous sinus stenosis. The average blood flow velocity and instantaneous blood flow rate at different phases were recorded. 3D streamlines represent the instantaneous blood-flow vector field for a single cardiac time frame and are used to visualize the spatial distribution and orientation of blood flow velocities. Color-coding by velocity magnitude facilitates the visual identification of regions with high systolic flow velocities. The color coding of the path lines reflect the magnitude of blood flow velocities in the vasculature (blue=low, red=high).Patient 1
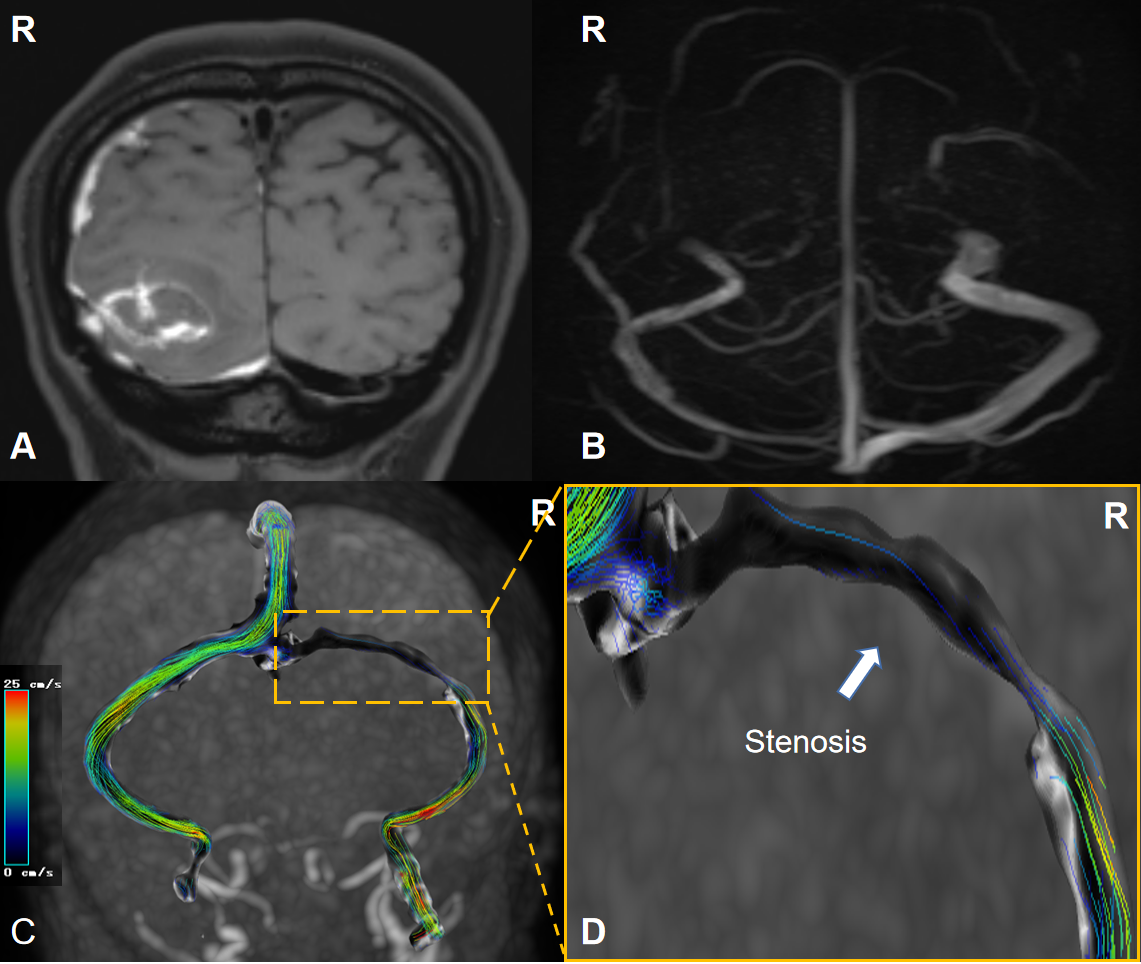
A 39 year old female with a clinical diagnosis of right cerebellar hemisphere hemorrhage and extensive subdural hematoma. MRV presented extrinsic stenosis which continuous in length owing to the extrinsic compression of right transverse sinus(Figure 1). The peak velocity of blood flow at stenosis, the proximal part and the distal part decreased, respectively 9.53cm/s, 33.38cm/s, 22.54cm/s . WSS which means the blood shear rate near the vessel wall peformed 0.02 Pa at stenosis. The lumen area at maximum stenosis is 26.8mm2.
Patient 2
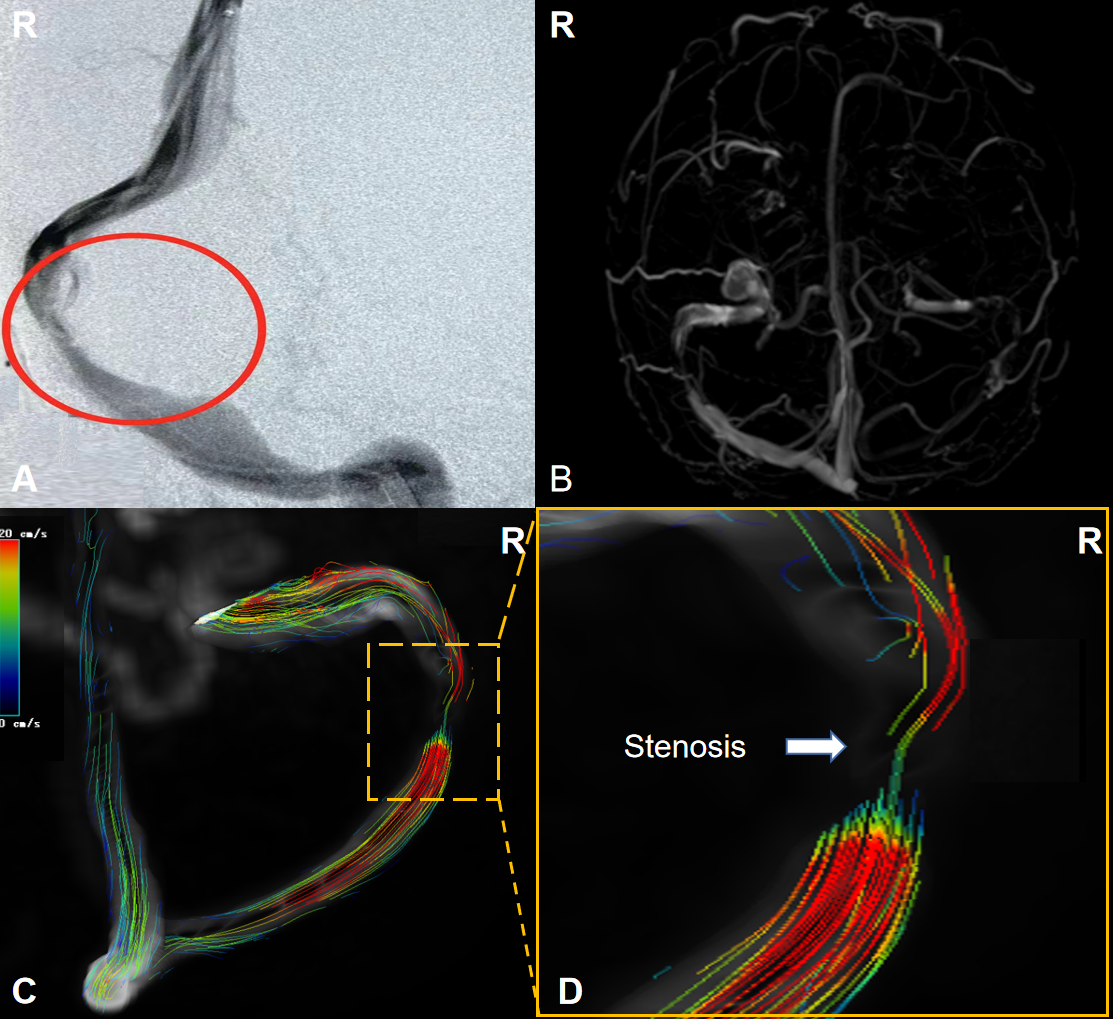
A 29-female presented with severe headache and papilledema with a clinical diagnosis of idiopathic intracranial hypertension. DSA and MRV showed the drainage dominance of right transverse sinus and right transverse sinus stenosis which confined a focal filling defect (Figure 2). The peak velocity of blood flow at stenosis, the proximal part and the distal part decreased, respectively 24.89cm/s, 36.24cm/s, 60.43cm/s. WSS peformed 0.11 Pa at stenosis.The lumen area at maximum stenosis is 18.4mm2.
Discussion
Routine MRI lacks quantitative hemodynamic information, conventional digital subtraction angiography (DSA) provides such data to a certain extent but invasive. 4D flow MRI can reflect the complex blood flow velocity and flow distribution in the blood vessels of interest1,2. 4D flow MRI permits flow volume quantification that is comparable to 2D PC MRI but has good scan-rescan repeatability. Further, 4D flow MRI measures velocity in all spatial directions, has superior spatial coverage, and has been shown to be better at capturing the peak velocity of a stenotic jet3. The findings demonstrate that venous sinus stenosis alter vascular flow dynamics in the stenosis area. For the severe venous sinus stenosis, regardless of the extrinsic or intrinsic factors, the peak velocities will decrease at the stenosis or the locations proximal and distal to the stenosis which compared with the normal data reported in the literature. At present, the study on the application of 4D flow MRI to the evaluation of intracranial hemodynamics is still in its infancy, but this technique has attracted increasing interest in the assessment of intracranial hemodynamics4.Conclusion
4D flow MRI has the potential to examine the entire cerebral venous system thus visualize and quantify hemodynamics in vivo for observation of blood flow pattern.Acknowledgements
No acknowledgement found.References
1. Soulat G, McCarthy P, Markl M. 4D Flow with MRI. Annu Rev Biomed Eng. 2020 Jun 4;22:103-126. doi: 10.1146/annurev-bioeng-100219-110055. Epub 2020 Mar 10. PMID: 32155346.
2. Wu C, Schnell S, Vakil P, Honarmand AR, Ansari SA, Carr J, Markl M, Prabhakaran S. In Vivo Assessment of the Impact of Regional Intracranial Atherosclerotic Lesions on Brain Arterial 3D Hemodynamics. AJNR Am J Neuroradiol. 2017 Mar;38(3):515-522. doi: 10.3174/ajnr.A5051. Epub 2017 Jan 5. PMID: 28057635; PMCID: PMC7959995.
3. Nordmeyer S, Riesenkampff E, Messroghli D, Kropf S, Nordmeyer J, Berger F, Kuehne T. Four-dimensional velocity-encoded magnetic resonance imaging improves blood flow quantification in patients with complex accelerated flow. J Magn Reson Imaging. 2013 Jan;37(1):208-16. doi: 10.1002/jmri.23793. Epub 2012 Sep 13. PMID: 22976284.
4. Schuchardt F, Hennemuth A, Schroeder L, Meckel S, Markl M, Wehrum T, Harloff A. Acute Cerebral Venous Thrombosis: Three-Dimensional Visualization and Quantification of Hemodynamic Alterations Using 4-Dimensional Flow Magnetic Resonance Imaging. Stroke. 2017 Mar;48(3):671-677. doi: 10.1161/STROKEAHA.116.015102. Epub 2017 Feb 8. PMID: 28179559.
Figures