2938
Accelerating brain susceptibility weighted imaging using compressed-SENSE1Beijing Tiantan Hospital, Capital Medical University, Beijing, China, 2Philips Healthcare, Beijing, China
Synopsis
Susceptibility weighted imaging (SWI), acquiring both magnitude and phase information for tissues using a 3D gradient-recalled echo sequence, is advantageous to detect microhemorrhages and microvasculature and useful in diagnosing small vessel diseases etc., but can be suffering from the long acquisition time. This study evaluated the effectiveness of brain SWI accelerated by compressed SENSE (CS-SENSE), and the CS-SENSE factor 4 is recommended in routine practice. Besides, the CS-SENSE factor 10 maybe a fast surrogate for distinguishing CMBs but sacrificing SN-RN visualizations.
Introduction
Susceptibility weighted imaging (SWI) acquires tissue signal with both magnitude and phase information using a 3D gradient-recalled echo sequence [1]. Despite of its wide applications in vessel imaging and hemorrhagic detection, SWI was limited by the long acquisition time which may lead to patient discomfort, motion artifacts and examination failure [2]. Compressed sensing (CS) technique was reported to be a promising acceleration method in brain MRI [3], while the effectiveness of CS accelerated SWI in clinical practice was under-studied, and the optimal CS acceleration factors in clinical examinations remains unclear. In this work, we aimed to evaluate the effectiveness of CS acceleration for SWI and identify the optimal CS acceleration factors for clinical practice. We systematically evaluated the image quality and diagnostic efficacy on cerebral microbleeds (CMBs) for CS-accelerated SWI with five different acceleration factors ranging from 2 to 10. These results were compared to the images acquired with a non-accelerated sequence.Methods
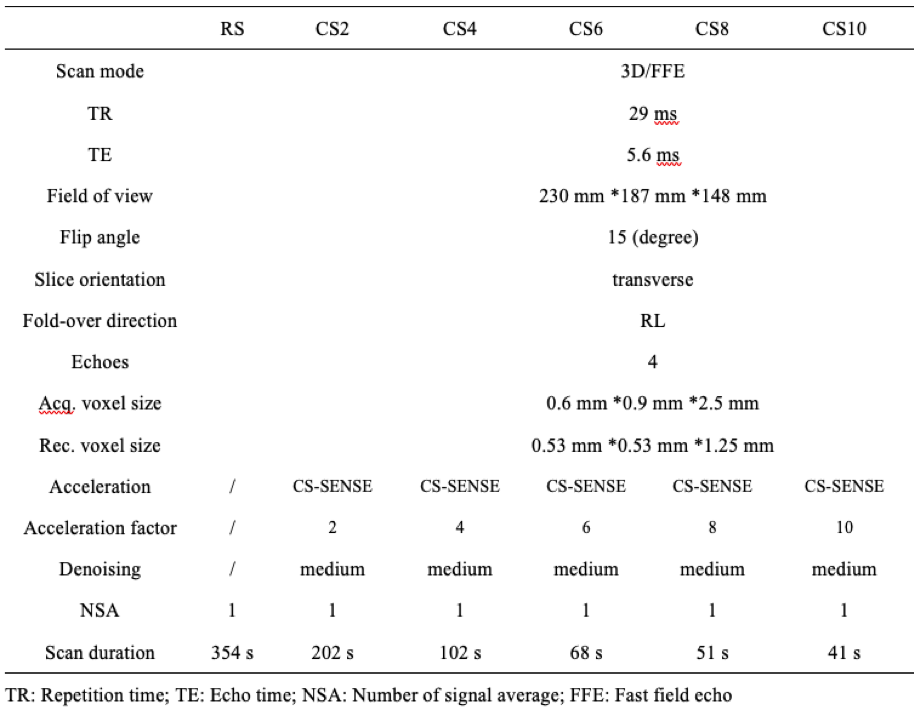
Ninety-nine subjects were scanned head-first in the supine position at 3.0 T where the same MR systems (Ingenia CX, Philips Healthcare) were installed with a 32-channel head coil and equipped with Compressed SENSE (a combination of CS and SENSE, hereafter referred as CS-SENSE) [4]. Six customized 3D SWI protocols were predesigned and optimized at Beijing Tiantan Hospital and then replicated at the MRI systems of other hospitals. Among the six protocols, five utilized CS-SENSE with acceleration factors of 2, 4, 6, 8, and 10 (denoted as CS2, CS4, CS6, CS8, and CS10, respectively); and one was a reference protocol without SENSE or CS-SENSE acceleration (denoted as RS). The parameters for the six SWI protocols are listed in Table 1. The image reconstruction was performed in real time during the scan. Quantitative measurements were performed on MATLAB R2016b (MathWorks). Signal intensities of RN and cerebrospinal fluid (CSF) were measured from the magnitude images for the calculation of signal to noise ratio (SNR) and contrast ratio (CR) based on regions of interest (ROIs) under the help of semi-automatic segmentation process supervised by two neuroradiologist. When drawing ROI for RN or CSF in one participant, equivalent size was chosen for the six protocols. The CSF measurements were mainly conducted on the lateral ventricle. Visual assessment was carried out by two neuroradiologists independently, blinded to the patient information and imaging parameters. The overall image quality, and the visibility of substantia nigra (SN) and RN (SN-RN) for all 6 protocols were assessed based on a five-grade scoring system.The interobserver reliability on quantitative measurements and visual assessment between the two neuroradiologists were assessed through Cohen’s kappa test. Repeated-measure ANOVA test would be performed to verify the difference of SNR and CR among the 6 sequences, and the Friedman test was used for the visual scores. Differences between each pair of protocols were evaluated by multiple comparisons with p values corrected by the Bonferroni correction. For all tests, p<0.05 was considered statistically significant.
Results
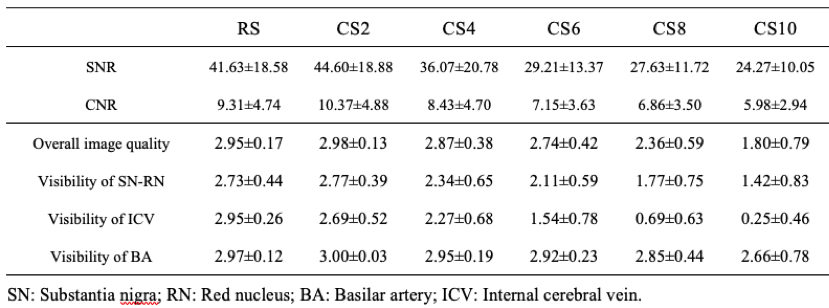
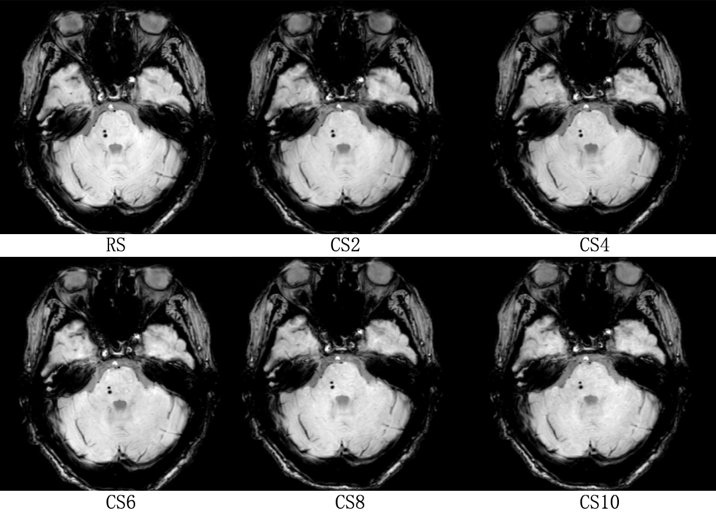
CS-SENSE technique showed a promising ability to reduce the acquisition time (from 202 s to 41 s) of SWI when increasing the acceleration factor from 2 to 10, although at the cost of decreasing SNR, CR, and the scores of visual assessments (Table 2). The visibility of the SN-RN became unacceptable in CS6 to CS10. The CMBs were well diagnosed in all CS-SENSE sequences (Figure 1). No significant difference was found for the detection or counting of the CMBs in 25 patients among the 6 SWI sequences, and the diagnosis for other intracranial lesions (cavernous angiomas: 3 cases, intracranial gliomas: 9 cases, and venous malformation: 5 cases) demonstrated 100% agreement either among the 6 SWI sequences or among the readers.Discussion and Conclusion
In this study, the CS-SENSE technique with 5 different acceleration factors was evaluated for brain SWI in a cohort of 99 patients. A reference sequence without acceleration was included for comparison. CS-SENSE with an acceleration factor of 10 was found as a feasible option for distinguishing the basilar artery, detecting the CMBs and providing valuable information on the diagnosis of cavernous angiomas, intracranial gliomas, venous malformation, and subacute hemorrhage. However, for better visualization of structures including both SN-RN and ICV, our result recommended the CS-SENSE factor not higher than 4.Acknowledgements
This work was supported by the National Science Foundation of China (Nos. 81870958 and 81571631), the Beijing Natural Science fund (No.7133244), the Beijing Nova Program (xx2013045).References
1. Haacke EM, Mittal S, Wu Z, et al. Susceptibility-weighted imaging: technical aspects and clinical applications, part 1. AJNR American journal of neuroradiology 2009;30:19-30
2. Holdsworth SJ, Yeom KW, Moseley ME, et al. Fast susceptibility-weighted imaging with three-dimensional short-axis propeller (SAP)-echo-planar imaging. Journal of magnetic resonance imaging : JMRI 2015;41:1447-1453
3. Wang N, Cofer G, Anderson RJ, et al. Accelerating quantitative susceptibility imaging acquisition using compressed sensing. Physics in medicine and biology 2018;63:245002
4. Ding J, Duan Y, Zhuo Z, et al. Acceleration of Brain TOF-MRA with Compressed Sensitivity Encoding: A Multicenter Clinical Study. AJNR American journal of neuroradiology 2021;42:1208-1215
Figures