2864
Acceleration Methods to Acquire Fast 3D Multi-Channel Absolute B1+ Maps at 7T for 8-Channel pTx1Wellcome Centre for Integrative Neuroimaging, FMRIB, Nuffield Department of Clinical Neurosciences, University of Oxford, Oxford, United Kingdom, 2Oxford Centre for Clinical Magnetic Resonance Research, University of Oxford, Oxford, United Kingdom, 3Department of Imaging Methods, Institute of Measurement Science, Slovak Academy of Sciences, Bratislava, Slovakia, 4Siemens Healthineers, Frimley, United Kingdom
Synopsis
Ultra-high field MRI with parallel transmit offers significant advantages but B1 transmit maps must be acquired to utilize its full potential. Acquiring absolute B1+ maps for each channel is a time-consuming process and limits the application of UHF to clinical practice. We compare two methods of accelerating the transmit mapping procedure to obtain fast volumetric multi-channel maps for an 8-channel transmit array. Both methods make use of a low-rank reconstruction (TxLR) from undersampled data and a modified pre-saturation TurboFLASH (satTFL) B1+ mapping sequence in combination with either Fourier encoding or a B1TIAMO style acquisition.
Introduction
Ultra-high field (UHF) MRI with parallel transmit offers significant advantages but B1 transmit maps must be acquired to utilize its full potential. Acquiring these absolute B1+ maps for each channel is a time-consuming process and limits clinical applications. TxLR1 has been shown to allow for high accelerations approximately equal to the number of transmit channels. We utilise this in combination with our recent work (in a parallel abstract) which reduces the acquisition time of pre-saturation B1+ mapping (satTFL2) by acquiring the reference and prepared images in quick succession (sat2TFL) and enabling significantly shorter TR’s. In this work we design and evaluated two methods of combining TxLR with sat2TFL to enable fast 3D multi-channel absolute maps of an 8-channel transmit array.Methods
The first acquisition strategy (Method A; Figure 1a) acquires 16 undersampled 3D absolute maps using Fourier encoded3 transmit configurations. Using linear combinations of transmit channels has been shown to overcome the issue of transmit sensitivity on the limited dynamic range of B1+ mapping methods and to supress erroneous measurements3. Secondly, we test an adaptation of B1TIAMO4 (Method B; Figure 1b) by acquiring eight undersampled 3D relative maps followed by two 3D absolute maps with complementary shim settings of CP and CP2. The individual channel maps for method B are calculated as described in the literature4. Each method acquires absolute maps using our sat2TFL sequence and undersampled data are jointly reconstructed using TxLR.Simulations using 2D synthetic body data, generated from Sim4Life 3.4 (ZMT, Switzerland), were performed to establish the optimal sampling strategy. Fully sampled data were generated using extended phase graph simulations for both methods. The images were then cropped in k-space, undersampled, and subsequently reconstructed according to each method. Additionally, we applied retrospective undersampling to fully sampled 2D data acquired with both methods.
Methods A and B were tested in phantom and in vivo on 3 volunteers to acquire 3D absolute single-channel maps using a 8Tx/32Rx head coil at 7T (Siemens). The reconstructed single-channel maps were compared to fully sampled 2D multi-transmit slices acquired using satTFL with a total acquisition time of 130s for the single slice. Acquisition matrices of 24×24×16 were undersampled using a variable density Poisson-disc mask. Nominal flip angles α/β of 9/90° with a 75V reference voltage. TurboFLASH TE/TR = 1.78/4.2ms, FOV = 250×250mm2, slice thickness = 10mm, bandwidth = 490Hz/px. Relative maps for method B were acquired using a gradient echo coil-cycled approach with TE/TR =5/13ms.
Results
The optimal sampling strategy, which enabled the most robust joint TxLR reconstruction (lowest RMSE), was found to be using the same undersampling mask per transmit configuration (as opposed to using unique or the same masks). Various undersampling factors using synthetic body data (Figure 2) show minimal error up to an undersampling factor of 6 compared to the fully sampled data. As expected, regions with the lowest transmit sensitivity show the greatest error, especially for method B using undersampling factors greater than 8 (Figure 2b). Retrospective undersampling shows similar results and undersampling factors of up to 8 are expected to be achievable in the brain (Figure 3). The 3D B1+ maps acquired using both methods in vivo are shown in Figure 4 and a comparison between the central partition and a 2D satTFL acquisition are shown in Figure 5.Discussion
There are trade-offs between the two methods demonstrated here; method B (B1TIAMO style) has the benefit of being more easily extended to larger transmit arrays. We found method A to be more robust to undersampling due to the over-determination of the encoding and down-weighting (based on the reference image) voxels with low transmit sensitivity. Figure 2 suggests method B is more suited to accelerated B1+ mapping in the heart, with accelerations of up to 6 achievable. Performance appears better in vivo (Figure 3) than in simulation likely due to a larger number of receive channels and improved transmit sensitivity in the brain. Our implementation of method B shown in Figure 5 consistently under-estimated B1+ when compared to the satTFL reference slice, whereas method A tended to over-estimate in regions of high α. The difference in performance between the 2D results presented in Figure 3 and the 3D results in Figures 4 and 5 are likely due to differences in the length of the readout train, requiring more careful bias-correction (see parallel abstract). Both methods may benefit from improved performance with further modifications, for example, more optimal undersampling strategies or sequence parameters.Conclusion
We obtain 3D single-channel absolute B1+ maps in the brain in under 18 seconds for an entire transmit array. This work is important to bring UHF to a more clinical audience by enabling faster B1+ mapping for tailored pTx.Acknowledgements
JK is supported by an iCASE stipend award in collaboration with Siemens Healthineers. LV is supported by a Sir Henry Dale Fellowship of the Wellcome Trust and the Royal Society [#221805/Z/20/Z] and would also like to acknowledge the support of the Slovak Grant Agencies VEGA [2/0003/20] and APVV [#19–0032]. The Wellcome Centre for Integrative Neuroimaging is supported by core funding from the Wellcome Trust (203139/Z/16/Z).
References
- Hess AT, Dragonu I, Chiew M. Accelerated calibrationless parallel transmit mapping using joint transmit and receive low‐rank tensor completion. Magn. Reson. Med. 2021;86:2454–2467.
- Chung S, Kim D, Breton E, Axel L. Rapid B 1 + mapping using a preconditioning RF pulse with TurboFLASH readout. Magn. Reson. Med. 2010;64:439–446.
- Tse DHY, Poole MS, Magill AW, Felder J, Brenner D, Jon Shah N. Encoding methods for B1+ mapping in parallel transmit systems at ultrahigh field. J. Magn. Reson. 2014;245:125–132.
- Brunheim S, Gratz M, Johst S, et al. Fast and accurate multi‐channel mapping based on the TIAMO technique for 7T UHF body MRI. Magn. Reson. Med. 2018;79:2652–2664.
Figures
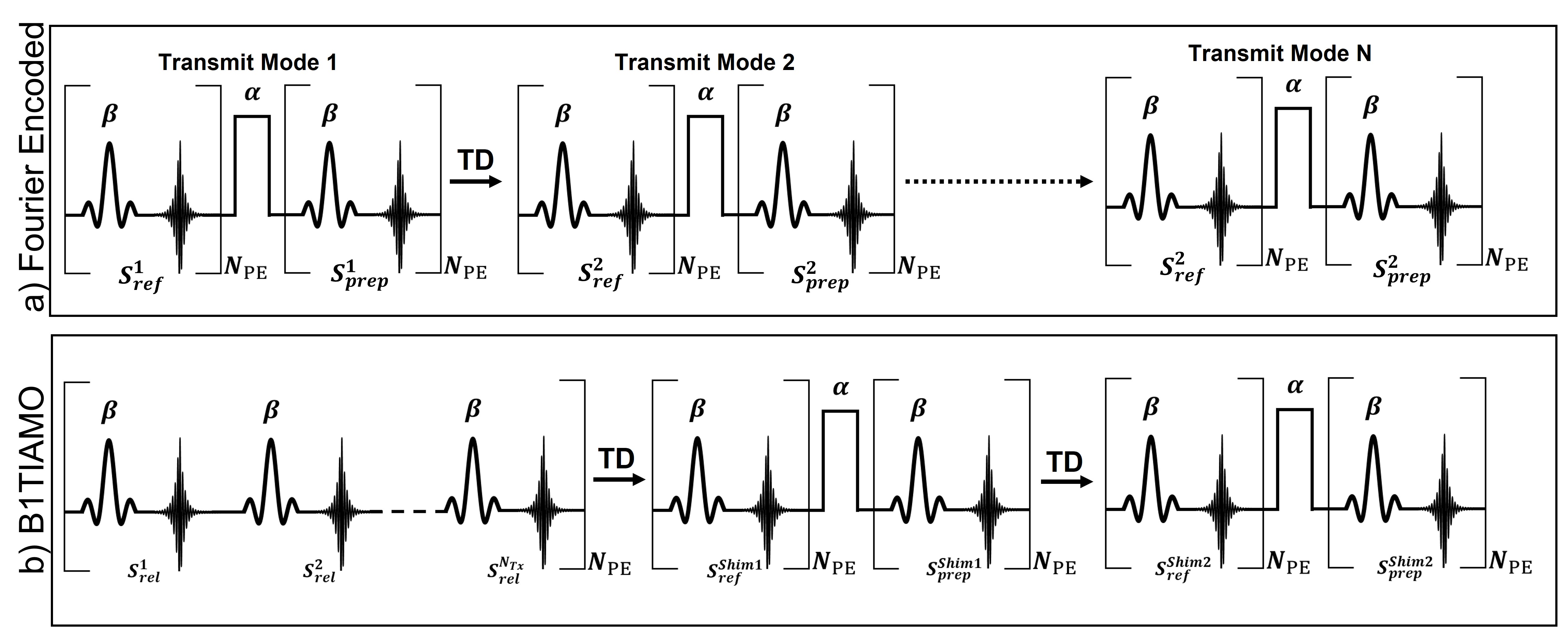
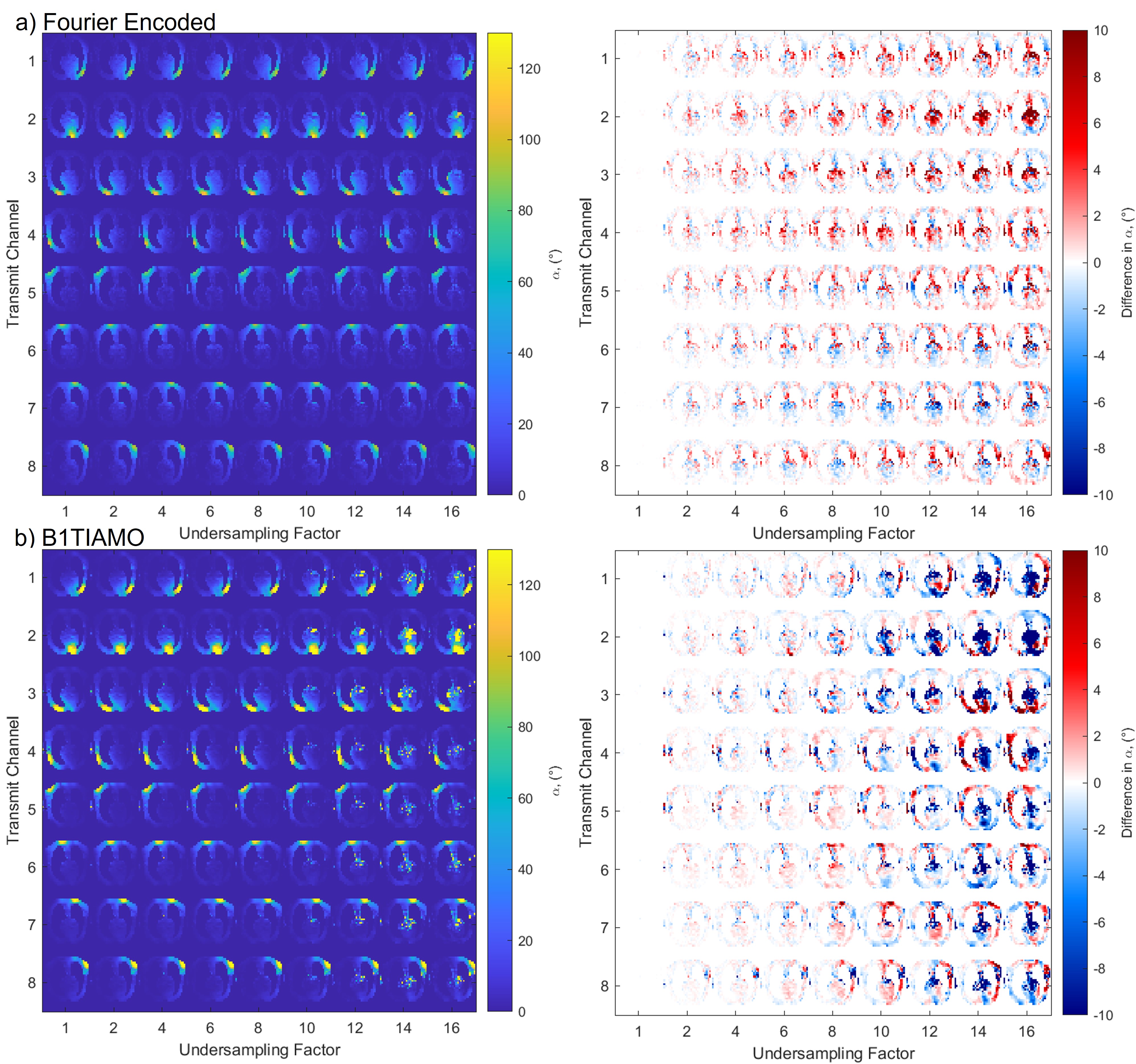
Figure 2: Retrospective under sampling of 2D synthetic body data (8Tx8Rx) for both the Fourier encoded method (a) and B1TIAMO method (b). Both the B1+ maps and error to the fully sampled maps are shown for different under sampling factors.
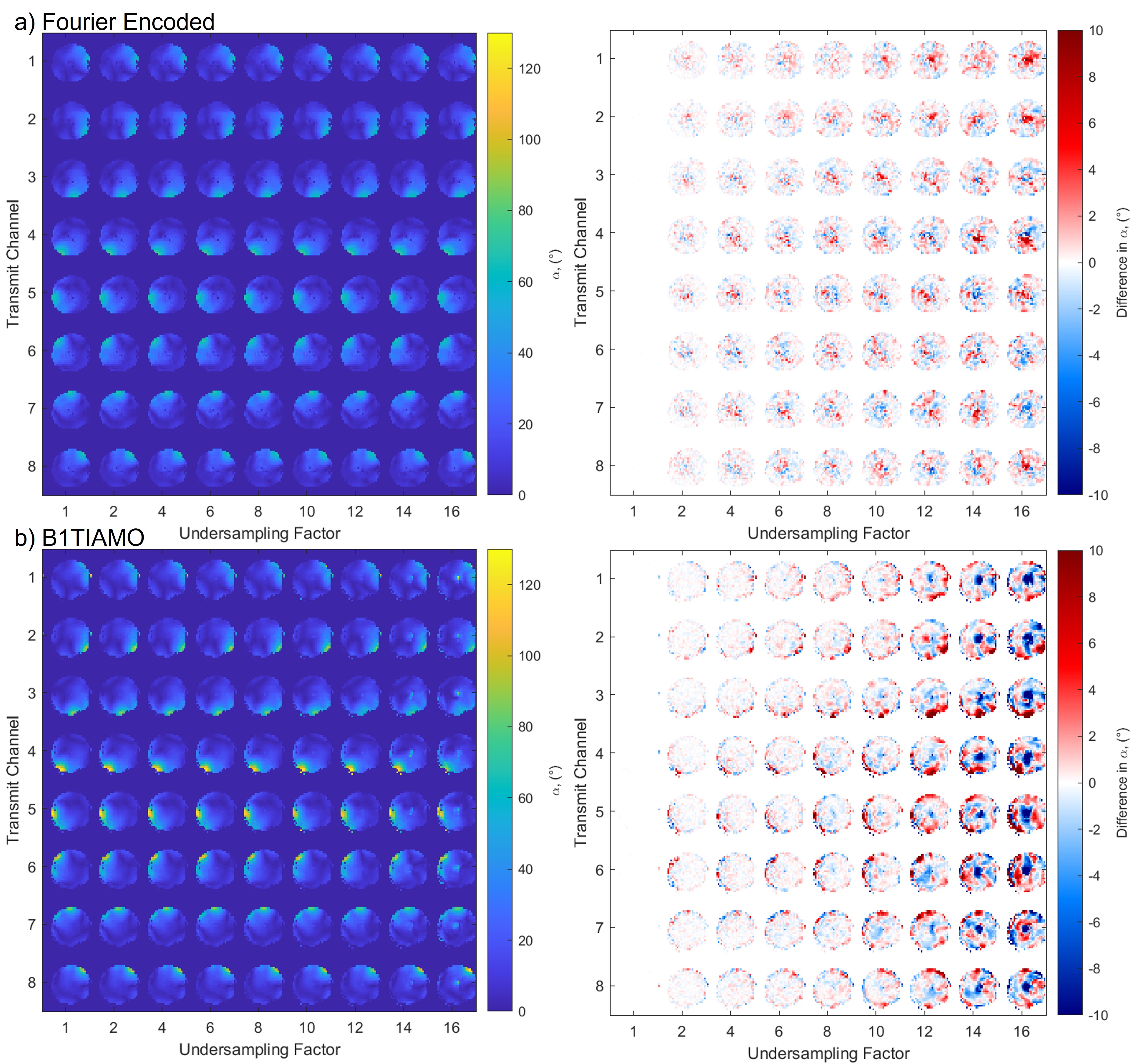
Figure 3: Retrospective undersampling applied to in vivo brain data for both the Fourier encoded method (a) and B1TIAMO method (b) with the difference to fully-sampled for various undersampling factors.
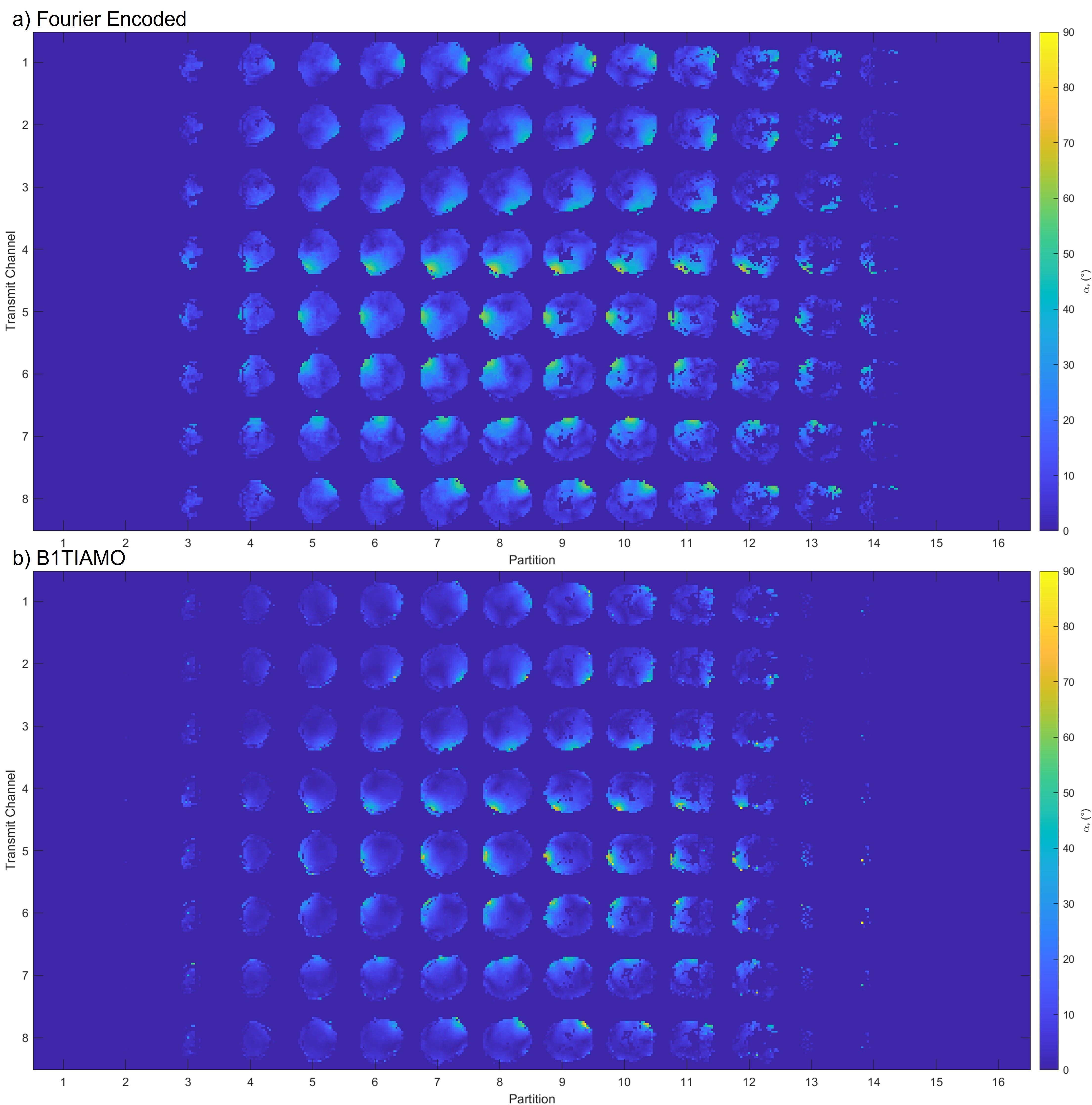
Figure 4: 3D absolute multi-channel B1+ maps acquired in the brain for the Fourier encoded method (a) and B1TIAMO style method (b) using an undersampling factor of 8. The acquisition time for (a) was 18 s and (b) 8 s.
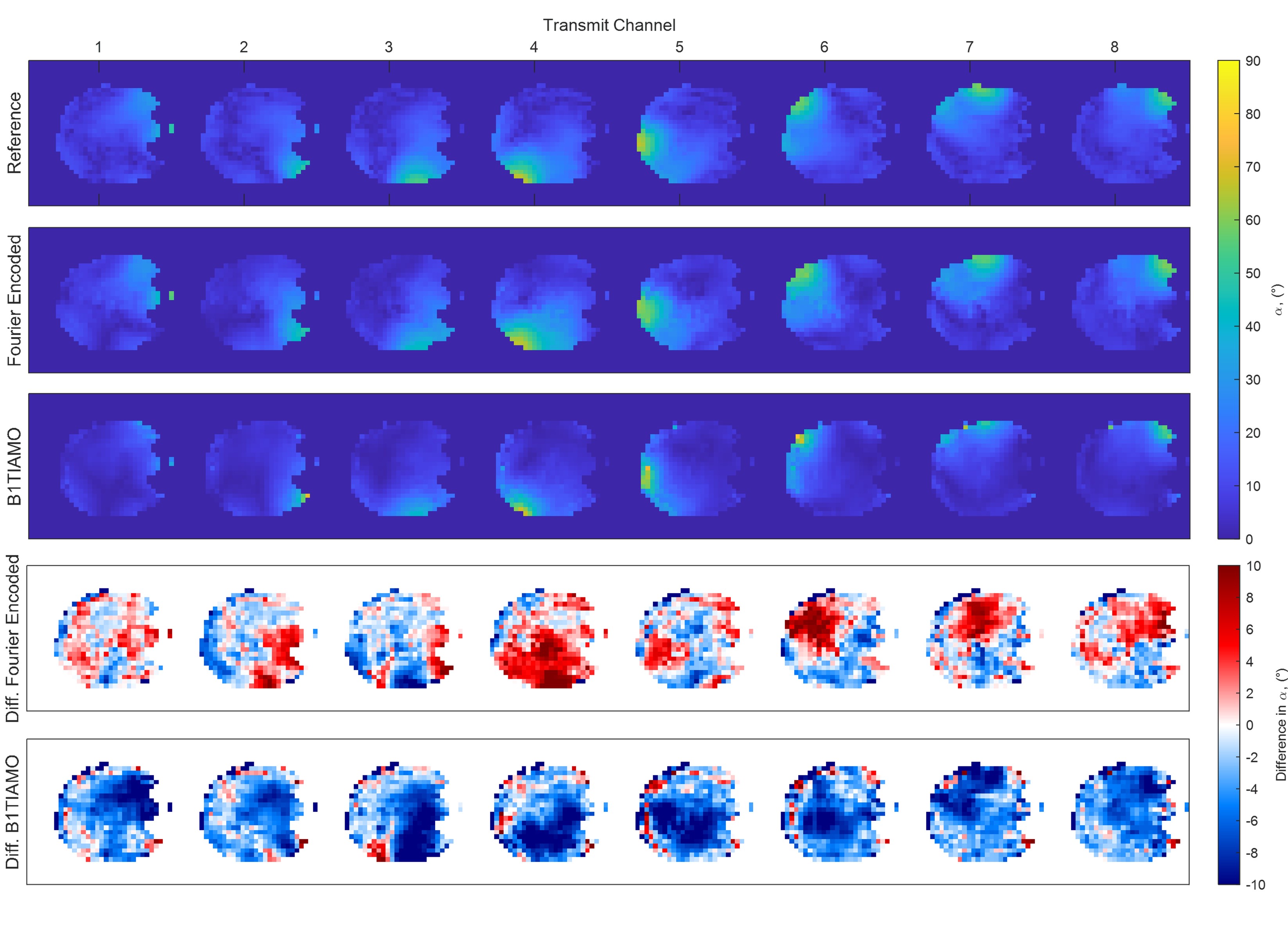
Figure 5: Centre partition B1+ maps from each 3D dataset acquired with either method A (Fourier encoded) or method B (B1TIAMO) compared to a 2D slice acquired using satTFL (130 s). The difference to the fully sampled 2D satTFL B1+ map is shown for each method in the both two rows.