2856
Native T1 Mapping Combined With Liver Stiffness Measurement in Identifying Significant Liver Fibrosis in Chronic Hepatitis B Patients1Department of Radiology, The Second Affiliated Hospital of Guangzhou University of Chinese Medicine, Guangdong Provincial Hospital of Traditional Chinese Medicine, Guangzhou, China, 2MR Scientific Marketing, SIEMENS Healthineers, Shanghai, China
Synopsis
Noninvasive identification of significant liver fibrosis in chronic hepatitis B patients is of great value because it can be an important indication for anti-viral therapy according to EASL guideline. This abstract was to evaluate the diagnostic capability of variable flip angle native T1 mapping combined with liver stiffness measurement (LT1 model) in identifying significant liver fibrosis in chronic hepatitis B patients. The LT1 score had good sensitivity and specificity for identifying significant liver fibrosis in chronic hepatitis B patients, and could provide a reliable basis for clinical diagnosis and treatment.
Objective
In order to evaluate the diagnostic capabilities of variable flip angle native T1 mapping combined with liver stiffness measurement (LSM) in identifying significant liver fibrosis in chronic hepatitis B (CHB) patients.Methods
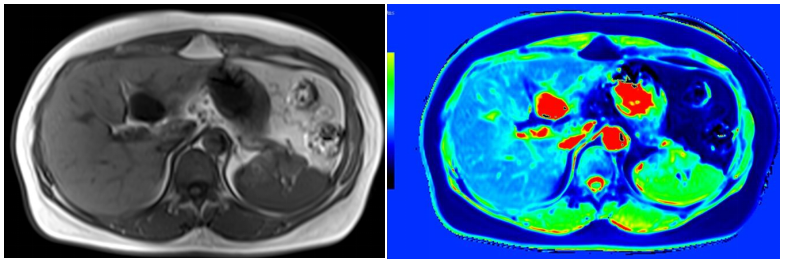
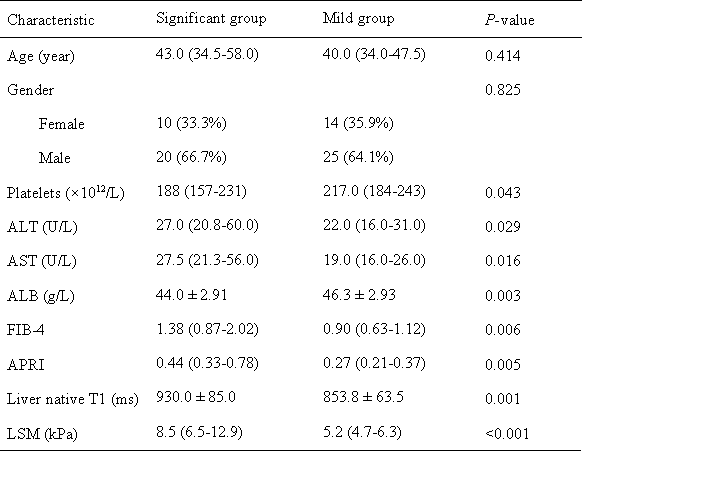
A total of 69 CHB patients (median age: 40 years old; interquartile range: 34–51 years; 45 men) were enrolled in this study, including 30 patients in the significant liver fibrosis group and 39 in the mild group. Patients who underwent transient elastography, variable flip angle native T1 mapping magnetic resonance imaging, and liver biopsy between December 2020 and June 2021 in our institute were retrospectively reviewed. According to liver biopsy based on the Batts-Ludwing scoring system, all enrolled patients were divided into two groups: significant group (liver fibrosis stage ≥ 2) and mild group (liver fibrosis stage < 2). Then clinical data and imaging features, including sex, age, platelets (PLT), aspartate transaminase (AST), alanine transaminase (ALT), albumin (ALB), AST to platelet ratio index (APRI), fibrosis-4 index (FIB-4), LSM and liver native T1 mapping were collected and statistically analyzed between two groups. Univariable and multivariable logistic regression analysis with forward stepwise selection was used to identify independent predictors and combined them for the construction of the significant group’s prediction scores. ROC curves were used to evaluate the diagnostic efficiency of the different indexes in identifying significant liver fibrosis. The Delong method was used to compare the differences among different ROCs.Results
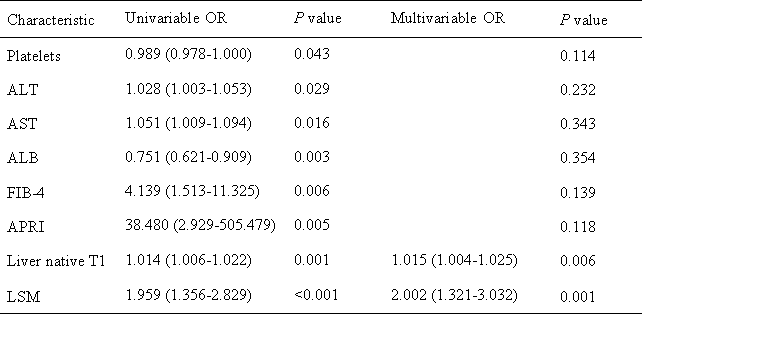
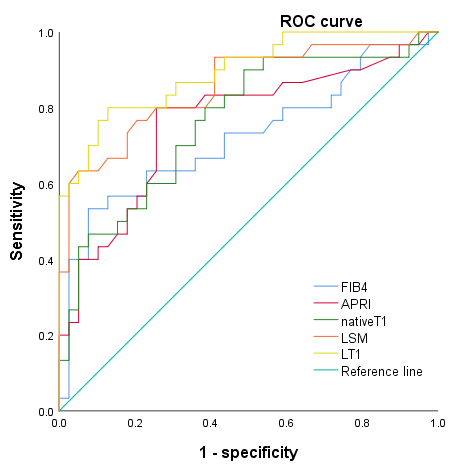
Univariate analysis showed that PLT, ALT, AST, ALB, APRI, FIB-4, LSM, and native liver T1 mapping had significant differences between these two groups. Multivariate logistic regression analysis showed that only LSM (odds ratio [OR]: 2.002; 95% CI: 1.321, 3.032; P = 0.001) and liver native T1 mapping (OR: 1.015; 95% CI: 1.004, 1.025; P = 0.006) were independent predictors for significant liver fibrosis. Based on the result of multivariate logistic regression analysis, an LT1 (LSM combined with liver native T1 mapping) score model was built as follows: LT1 = 0.694*LSM + 0.015*T1 - 18.064. The AUC of LT1, LSM, liver native T1 mapping, APRI, and FIB-4’s ROCs in identifying significant liver fibrosis were 0.895, 0.855, 0.764,0.722, and 0.760, respectively. The diagnostic capability of LT1 was apparently superior to native T1 mapping, APRI, and FIB-4 (P = 0.012, 0.023, and 0.013), but there was no significant difference between LT1 and LSM (P = 0.226). Using the cutoff value of 0.036, the sensitivity and specificity of the LT1 score model in identifying significant liver fibrosis were 0.80 and 0.87, respectively.Conclusion
Variable flip angle native T1 mapping combined with liver stiffness measurement could effectively identify significant liver fibrosis in chronic hepatitis B patients. The diagnostic capability of the LT1 score model was superior to LSM, liver native T1 mapping, APRI, and FIB-4. Using a proper cutoff value, the LT1 score showed favorable sensitivity and specificity, which may provide helpful and reliable evidence for clinical decision-making and treatment.Acknowledgements
No acknowledgement found.References
1. European Association for the Study of the Liver. European Association for the Study of the Liver. EASL 2017 Clinical Practice Guidelines on the management of hepatitis B virus infection. J Hepatol. 2017 Aug;67(2):370-398.
2. Goodman ZD. Grading and staging systems for inflammation and fibrosis in chronic liver diseases. J Hepatol. 2007 Oct;47(4):598-607.
3. Li J, Liu H, Zhang C, Yang S, Wang Y, Chen W, Li X, Wang D. Native T1 mapping compared to ultrasound elastography for staging and monitoring liver fibrosis: an animal study of repeatability, reproducibility, and accuracy. Eur Radiol. 2020 Jan;30(1):337-345.
4. Qi X, An M, Wu T, Jiang D, Peng M, Wang W, Wang J, Zhang C, Chess Study Group OBOT. Transient Elastography for Significant Liver Fibrosis and Cirrhosis in Chronic Hepatitis B: A Meta-Analysis. Can J Gastroenterol Hepatol. 2018 May 24;2018:3406789.
Figures