2671
Ex vivo 7T MRI of resection specimen of oral cancer to improve margin control.1Head and Neck Surgical Oncology, University Medical Center Utrecht, Utrecht, Netherlands, 2Biomedical MR Imaging & Spectroscopy Group, University Medical Center Utrecht, Utrecht, Netherlands, 3Pathology, University Medical Center Utrecht, Utrecht, Netherlands, 4Radiology, University Medical Center Utrecht, Utrecht, Netherlands, 5Radiotherapy, University Medical Center Utrecht, Utrecht, Netherlands
Synopsis
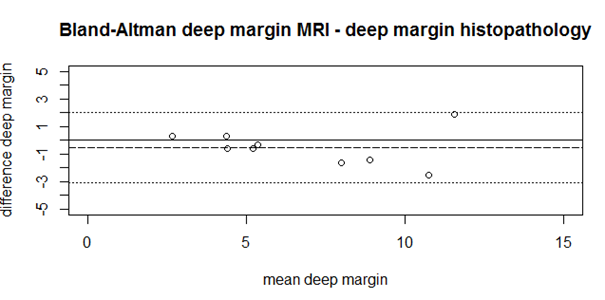
We validated the measured resection margins of the surgical specimens of tongue carcinoma on 7T ex vivo MRI with histopathology using T2 weighted MRI. In 3D T2wTSE (250 μm3) with an acquisition time of 15-20 minutes, the resection margins was undestimated by 0.5 mm (+/- 1.3 mm). This will be developed into a clinical study with immediate re-resection during surgery to prevent adjuvant (chemo)radiotherapy, which is associated with radiation induced side effects.
introduction
Oral squamous cell carcinoma (OSCC) is preferably treated by surgery. Its complete removal is essential for locoregional control and disease-free survival. Inadequate resection margins require adjuvant therapy such as re-resection or (chemo)radiation, which causes extra morbidity. In international literature, 30% to 85% inadequate resection margins are reported [1]. For tongue SCC, both intraoral ultrasonography (US) and magnetic resonance imaging (MRI) are reported to be very accurate in determining tumor thickness and depth of invasion preoperatively. In addition to in vivo imaging, also ex vivo imaging can help to improve the number of adequate resections. Since 7T MRI has the potential to visualize fine details, ex vivo 7T MRI of the resection specimen of OSCC can indicate areas with close or positive resection margins for immediate re-resection [2] and by that reduce adjuvant radiotherapy treatment and eventually improve oral function and the patient’s quality of life by adequate tumor resection.aim
A feasibility study to optimize the MRI protocol was performed in tongue tumors and compared to histopathology to build experience with ex vivo 7T MRI of resection specimen of OSCC in 10 tongue cancer patients.Material and Methods
Ex vivo MR imaging of resection specimens was performed on a Bruker 7T MR spectrometer (BioSpec7T, Bruker, Ettlingen, Germany) interfaced with a Philips console. Multislice T2w TSE images (in plane 125 μm2 slice thickness 1 mm), 3D T2w TSE (250 μm3) and DTI was performed (b-values: 0, 800, 1600 and 3200 s/mm2, 40 directions, 1 mm3). The tumor thickness and the smallest resection margins were measured in the MR images. Hematoxylin and eosin stained sections were cut every 3-5 mm and the distance between tumor outline and resection edge was measured and compared with the resection margins on MRI. In addition, MRI and histology was spatially correlated.Results
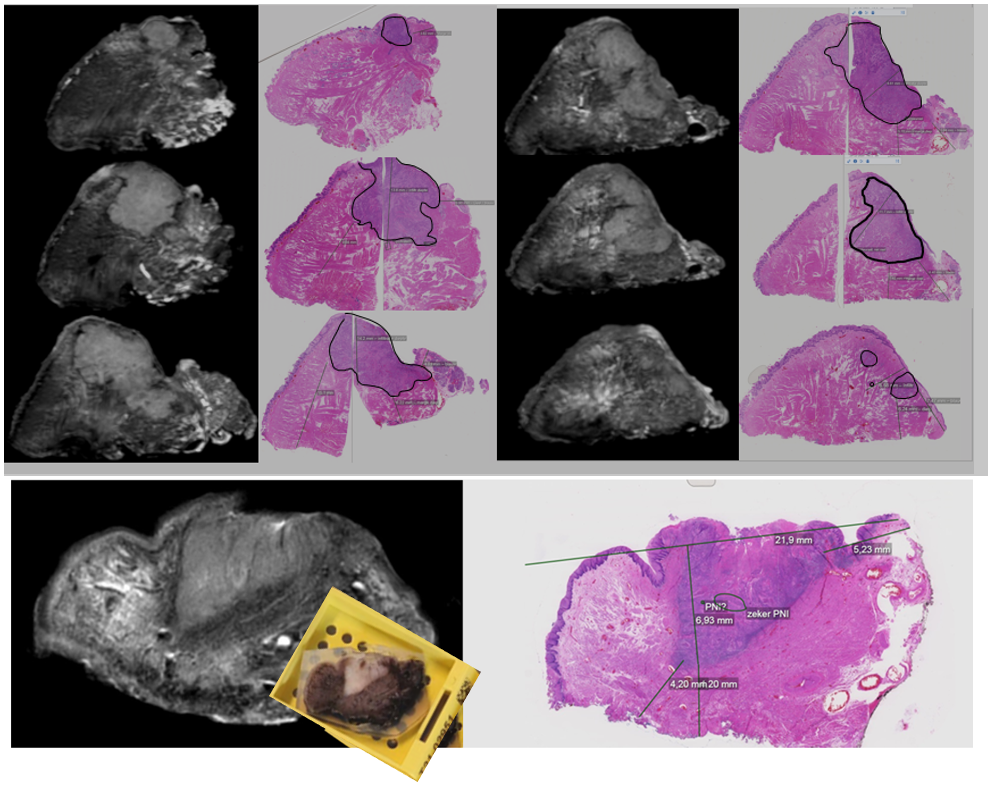
HE stained sections and 7T MRI were compared and showed a small over-estimation of tumor thickness on MRI versus histopathology (1.2±1.0mm), while it slightly under-estimated the margin (0.5±1.2mm) (Figure 1). In addition, the tumor on HE stained sections and 3D T2 weighted TSE images were reoriented to match the histopathological sagittal slices and visually tumor extent on both 3D and multislice T2 weighted images (Figure 2). DWI showed acceptable co-localization with histopathology. Muscle fiber tracking showed the directionality of muslce fibers in the tongue. The total scan time of the three images was 30 – 45 minutes, depending on the size of the specimen.Discussion and conclusion
The resection margins and tumor thickness on 7T MRI differed only slightly from that on histopathology. As the time for evaluation during surgery for immediate re-resection has to be limited, acquisition time and evaluation time has to be within 45 minutes, which means that maximum imaging time will be limited to 20-30 minutes. Therefore, either accelerated image acquisition is needed or only a single MR contrast and acquisition has to be chosen. For optimal 3D spatial correlation some refining using only whole mount sectioning and automatic registration between whole mount sections and MR images is desirable.In conclusion, the close agreement between histopathology and 7T T2w images is promising for the transfer of ex vivo 7T MRI to a clinical study.
Acknowledgements
We thank Tijl van der Velden for the technical assistance on the 7T scanner, Gerard van Vliet for the daily support and Martijn Foeling for setting up and processing of the muscle DTI.References
1. Smits, R. W., Koljenović, S., Hardillo, J. A.,Ten Hove, I., Meeuwis, C. A.,Sewnaik, A., Dronkers, E. A., Bakker Schut, T. C., Langeveld, T. P., Molenaar, J., Hegt, V. N., Puppels, G. J. & Baaenburg de Jong, R. J. 2016.Resection margins in oral cancer surgery: Room for improvement. Head Neck, 38 Suppl 1, E2197-203.
2. Steens, S. C. A., Bekers, E. M., Weijs, W. L. J., Litjens, G. J. S., Veltien, A.,Maat, A., van den Broek, G. B., van der Laak, J. A. W. M., Futterer, J. J., vander Kaa, C. A. H., Merkx, M. A. W. & Takes, R. P. 2017. Evaluation of tonguesquamous cell carcinoma resection margins using ex-vivo MR. Int J Comput Assist RadiolSurg, 12, 821-828.
Figures