2556
Local SAR management strategies for RF shimming in fetal MRI at 3T1Fetal-Neonatal Neuroimaging and Developmental Science Center, Boston Children's Hospital, Boston, MA, United States, 2Department of Pediatrics, Boston Children's Hospital, Boston, MA, United States, 3Department of Electrical Engineering and Computer Science, Massachusetts Institute of Technology, Cambridge, MA, United States, 4Harvard-MIT Health Sciences and Technology, Cambridge, MA, United States, 5Institute for Medical Engineering and Science, Massachusetts Institute of Technology, Boston, MA, United States, 6Department of Radiology, Boston Children's Hospital, Boston, MA, United States, 7Athinoula A. Martinos Center for Biomedical Imaging, Harvard Medical School, Boston, MA, United States, 8Department of Radiology, Massachusetts General Hospital, Boston, MA, United States
Synopsis
RF shimming (RFS) improves the transmit field for fetal MRI, however, fetal safety is understudied. Previous simulations studied the SARlocal of the standard imaging mode (CP mode) of each subject to inform the safety of RFS. We evaluated two local SAR management strategies which utilize subject-specific models and use either the individual’s CP mode SARlocal as a limit for RFS or the maximum CP mode SARlocal value across 7 subjects. We evaluated the B1+ performance inside the fetus for each strategy. Using the maximum CP mode SARlocal across the population as the SAR limit greatly improves RFS performance.
Target audience
MR physicists and clinicians interested in using RF shimming in fetal MRI at 3T.Introduction
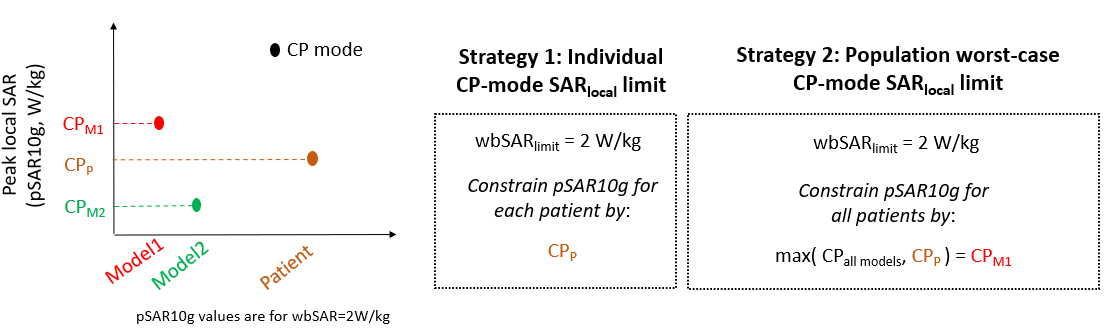
RF shimming (RFS) can improve fetal MRI excitation leading to increased signal and more uniform contrast at 3T.1–3 However, RFS can also increase local SAR, raising safety concerns.1–3 The International Electrotechnical Commission (IEC) recommends scanning pregnant subjects in normal operating mode (maternal whole-body SAR=2W/kg) but otherwise do not specify limits on fetal SAR.4 For this reason, previous fetal RFS studies analyzed the effect on excitation metrics when SARlocal was limited to that found in the standard mode of imaging, the circularly polarized (CP) birdcage mode, in that individual’s body model.1,2 In this scenario, the individual defines their own safety limit using the assumption that SAR hotspots resulting from CP-mode imaging limited to SARwhole-body≤2W/kg is safe. This is intrinsically different from SARlocal limits for RFS in nonpregnant subjects since it results in a different SAR limit for each patient. Although acceptable, this approach is conservative for subjects who happen to have low CP-mode SARlocal. For example, if patient A’s model shows a CP mode SARlocal=15 W/kg and patient B’s model shows 30 W/kg, the higher SARlocal would be deemed safe in patient B but not A. A less conservative approach would be to take the population worst-case CP-mode SARlocal and conclude that this value is safe in all patients because CP-mode imaging is widely used in a range of patients.In this study, we evaluate two local SAR management strategies for fetal RFS and calculate the resulting B1+ performance inside the fetus across 7 numerical pregnant body models. In both strategies, fetal and maternal SARlocal is determined using subject-specific modelling and used to constrain RFS. In the first strategy, we use the individual’s CP-mode SARlocal as the SAR limit in RFS, as in previous studies. For the second strategy, we use the maximum CP-mode SARlocal value across the 7 models as the SAR limit in RFS. Finally, we run thermal simulations to compare the temperature increase of CP-mode and RFS.
Methods
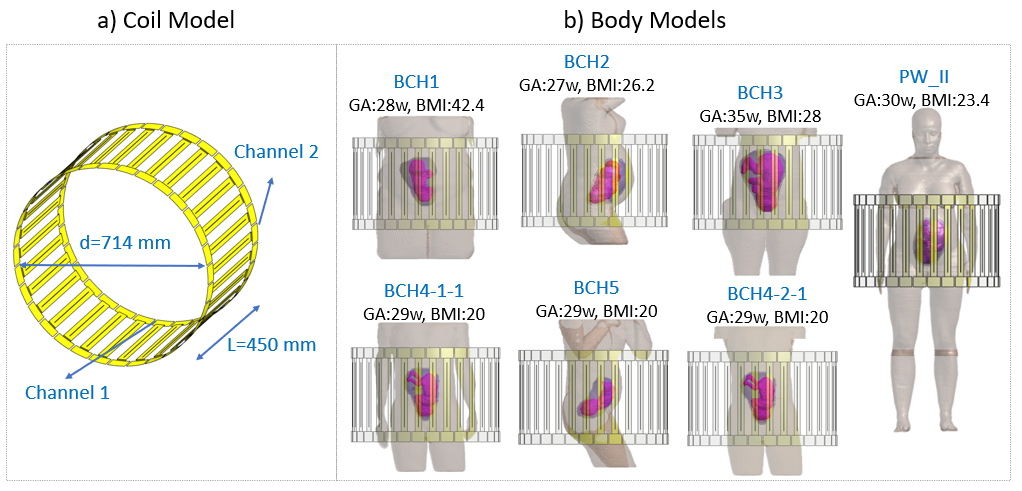
EM simulations: We evaluate the local SAR management strategies in seven numerical pregnant body models5–7 (Fig.1) in a 2-port 32-rung high-pass birdcage coil model. Electromagnetic simulations were run in Sim4Life (Zurich MedTech, Zurich, Switzerland) to calculate B1+ and SAR in each model.Local SAR management: Two strategies, both of which constrain local SAR using subject-specific SAR models, were evaluated for each ‘patient’ in terms of the resulting RFS |B1+| average and variation inside the fetus. Strategy 1 (Individual CP-mode SARlocal limit): uses each patient’s CP-mode SARlocal as their SARlocal limit in RFS. Strategy 2 (population worst-case CP-mode SARlocal limit): uses the maximum CP mode SARlocal value across the population as the SARlocal limit in RFS. These strategies were simulated by selecting one of the body models as the ‘patient’ and the rest of the models as the population (for Strategy 2).
RF shimming: An exhaustive search was carried out to find the best RF shim setting (without SAR constraints) and the optimal RF shim settings for each Strategy. For the search space, relative amplitude and phase of the two ports was varied from 0 to 2 and -90° to 270° in steps of 0.1 and 10°, respectively. Maternal 10g average peak local SAR (pSAR10g), fetal pSAR10g and fetal average SAR (aveSAR) was constrained in the local SAR management process. Average |B1+| and coefficient of variation (CV) of |B1+| inside the fetus were compared between the CP mode, best shim settings and the optimal shim settings for Strategy 1 and 2. All values were normalized to 2W/kg maternal whole-body SAR (wbSAR).
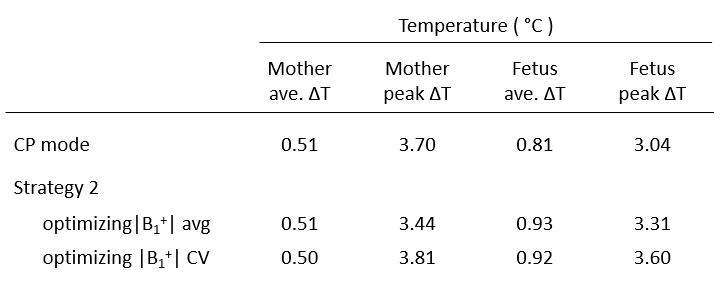
Thermal simulations: We compare maximum temperature increase (ΔT) across models after 30 minutes of exposure to 2 W/kg wbSAR for CP mode and the optimal shim settings resulting from Strategy 2.
Results
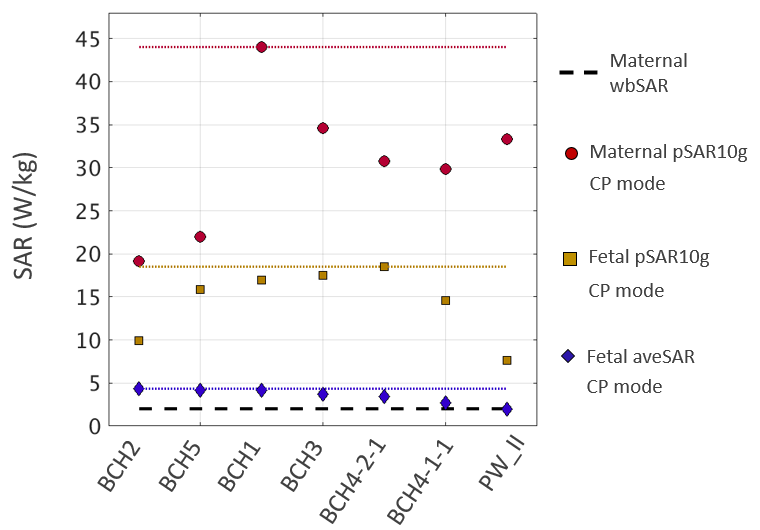
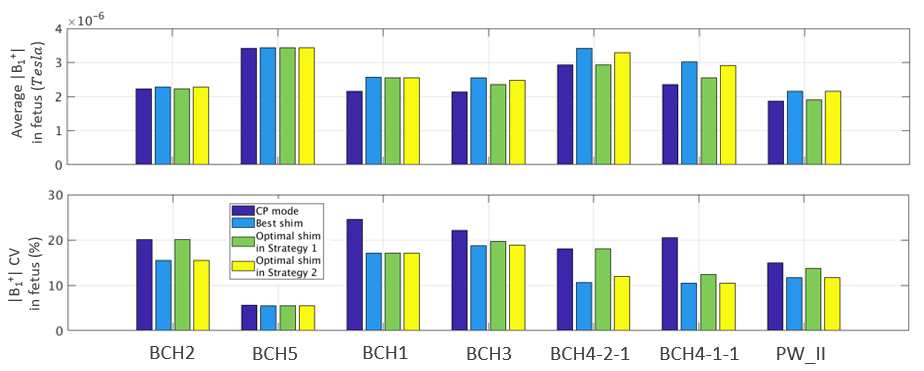
Figure 3 shows fetal and maternal SAR for the CP mode across 7 models. Point shape/colors depict the local SAR limits in Strategy 1 while the dashed lines indicate the worst-case values used in Strategy 2. Figure 4 shows |B1+| average and CV across all models for CP mode, best shim settings, and optimal shim settings resulting from the 2 strategies. The average improvements across models in |B1+| average and CV compared to CP mode are 15% and 26% for best shim settings, 6% and 13% when RFS is constrained by Strategy 1, and 13% and 25% when RFS is constrained by Strategy 2. Maximum ΔT observed with Strategy 2 is up to 18% higher compared to CP mode as shown in Table 1.Discussion
This study shows that using SARlocal limits from the maximum CP-mode SARlocal values in the population instead of each patient’s own CP-mode SARlocal greatly improves the transmit field performance of 2-channel RF shimming. Thermal simulations show that maximum ΔT across the population is within 18% of those in CP mode. Future work includes assessing the locations of maximum ΔT for different excitation modes and running thermal simulations for realistic scan scenarios instead of constant 2 W/kg exposure.Acknowledgements
This work was supported by R01HD100009, U01HD087211, R01EB017337, and R01EB006847.References
1. Yetisir F, Abaci Turk E, Guerin B, et al. Safety and imaging performance of two-channel RF shimming for fetal MRI at 3T. Magn Reson Med. 2021;86(5):2810-2821.
2. Murbach M, Neufeld E, Samaras T, et al. Pregnant women models analyzed for RF exposure and temperature increase in 3T RF shimmed birdcages. Magn Reson Med. 2017;77(5):2048-2056.
3. Filippi C, Johnson A, Nickerson J, Sussman B, Gonyea J, Andrews T. Fetal Imaging with Multitransmit MR at 3.0T: Preliminary Findings. In: Proceedings of the 18th Annual Meeting of ISMRM. Stockholm, Sweden. 2010, p2023.
4. International Electrotechnical Commission. IEC 60601-2-33: Medical electrical equipment-Particular requirements for the basic safety and essential performance of magnetic resonance equipment for medical diagnosis. https://webstore.iec.ch/publication/22705. Published 2015. Accessed April 22, 2021.
5. Abaci Turk E, Yetisir F, Adalsteinsson E, et al. Individual variation in simulated fetal SAR assessed in multiple body models. Magn Reson Med. 2020;83(4):1418-1428.
6. Christ A, Kainz W, Hahn EG, et al. The Virtual Family—development of surface-based anatomical models of two adults and two children for dosimetric simulations. Phys Med Biol. 2010;55(2):N23-N38.
7. Gosselin MC, Neufeld E, Moser H, et al. Development of a new generation of high-resolution anatomical models for medical device evaluation: the Virtual Population 3.0. Phys Med Biol. 2014;59(18):5287-5303.
Figures