2512
Evaluation of multiband variable-rate selective excitation (MB-VERSE) diffusion-weighted imaging (DWI) of the liver MRI1Radiology, Severance Hospital, Research Institute of Radiological Science, Yonsei University College of Medicine, Seoul, Korea, Republic of
Synopsis
In liver MRI, diffusion-weighted imaging (DWI) allows better detection and characterization of focal lesions, but requires a relatively long scan time. The multiband variable-rate selective excitation (MB-VERSE) echoplanar imaging for DWI provides accelerated acquisition time with some expected trade-off in image quality. Qualitative and quantitative image quality of MB-VERSE images as well as focal liver lesion detectability was evaluated by three readers. The MB-VERSE sequence as well as focal liver lesion detectability showed significant sacrifice in quantitative and qualitative overall image quality, but comparable focal lesion detectability.
Introduction
In liver MR, diffusion-weighted imaging (DWI) allows better detection and characterization of focal lesions, but requires a relatively long scan time. The multiband variable-rate selective excitation (MB-VERSE) echoplanar imaging for DWI of the liver provides accelerated acquisition time with some expected trade-off in image quality.1,2 The purpose of this study was to evaluate the qualitative and quantitative image quality as well as focal liver lesion detectability of MB-VERSE DWI of the liver.Methods
Between October and December of 2020, a total of 144 consecutive patients who underwent liver or pancreaticobiliary MR were included for retrospective analysis. Both conventional DWI and MB-VERSE DWI were acquired without breath hold. Image quality was evaluated both qualitatively (overall image quality, sharpness of liver margin, image quality at liver dome, degree of artifacts, and focal lesion conspicuity) and quantitatively (signal-to-noise ratio (SNR), contrast-to-noise ratio (CNR), and apparent diffusion coefficient (ADC) values).3,4 Image quality parameters were compared using the Wilcoxon signed rank test. Agreeability of ADC value of both liver and focal liver lesions were analyzed using the Bland-Altman plot. Mean diagnostic accuracy for focal lesion detectability was calculated according to the mean figure-of-merit (FOM) from the area under the jackknife alternative free-response receiver operating characteristic (JAFROC) curve.5Results
The MB-VERSE DWI showed significantly shorter scan time compared to that of the conventional DWI (99.0 seconds versus 133.0 seconds, p < 0.001). Qualitative image quality parameters were all poorer for MB-VERSE DWI compared to the conventional DWI (all p < 0.05). The MB-VERSE DWI showed significantly lower SNR (34.9 versus 50.0, p < 0.001), but comparable CNR (57.5 versus 78.9, p = 0.070) compared to the conventional DWI. The ADC values of the liver parenchyma was significantly lower in the MB-VERSE DWI (p = 0.012). The Bland-Altman plot showed that the ADC value of the liver parenchyma on the MB-VERSE DWI was lower than that of the conventional DWI (bias, 0.09 ×10-3 mm2/s) with limits of agreement (LOA) ranging from -0.51 to 0.68 ×10-3 mm2/s. On the other hand, the ADC value of focal lesions in the MB-VERSE DWI were slightly higher than that of the conventional DWI (bias, -0.17 ×10-3 mm2/s) with LOA ranging from -1.37 to 1.02 ×10-3 mm2/s, but without statistical significance (p = 0.346).Discussion
The MB-VERSE DWI significantly reduces scan time with some sacrifice in overall image quality, cutting acquisition time by 23.4% with only 15.6% decrease in SNR. Despite the trade-off of image quality, CNR and focal lesion detectability of focal liver lesions on MB-VERSE DWI were comparable to those on the conventional DWI.The significant reduction of scan time of the MB-VERSE DWI was accompanied by significant sacrifice of SNR, but not CNR. This may be due to the greater loss of signal of the liver parenchyma compared to the loss of signal of the focal lesion or background noise level. As a result, despite the lower SNR, poorer subjective image quality, poorer focal lesion conspicuity, and more severe artifacts, both per lesion and per patient focal lesion detectability on MB-VERSE DWI was non-inferior to that of the conventional DWI.
The ADC values of liver parenchyma on MB-VERSE DWI were significantly lower than that of the conventional DWI by 0.09 ×10-3 mm2/s, with shorter TR of the MB-VERSE DWI than of the conventional DWI (1609.0 ms versus 3226.4 ms, respectively).6,7 On the other hand, ADC value of focal liver lesions were slightly higher on MB-VERSE DWI than on conventional DWI, although without statistical significance (p = 0.346), which may be the reason for the comparable CNR and focal lesion detectability between the two DWI techniques.
The MB-VERSE DWI showed comparable focal liver lesion detectability to the conventional DWI. Although this is promising for future clinical application, it is undeniable that overall poorer image quality and poorer focal lesion conspicuity may lead to longer interpretation time and stress on the radiologist’s part. Therefore, further optimization of the MB-VERSE DWI is warranted to minimize the trade-off of image quality with possibly higher acceleration factor with relatively preserved image quality and focal lesion detectability.
Conclusion
The MB-VERSE DWI significantly reduced scan time with some sacrifice in overall image quality, but with preserved focal lesion detectability. Further optimization of the MB-VERSE DWI technique is required to yield improved image quality with shorter scan time.Acknowledgements
No acknowledgement found.References
1. Barth, M., Breuer, F., Koopmans, P. J., Norris, D. G. & Poser, B. A. Simultaneous multislice (SMS) imaging techniques. Magnetic resonance in medicine 75, 63-81 (2016).
2. Kosuke Morita et al. MultiBand-SENSE EPI with Variable-Rate Selective Excitation (VERSE) pulses for accelerating abdominal DWI with respiratory triggering in Proceedings of the Annual Meeting of ISMRM 2021).
3. Xu, J. et al. Simultaneous multi-slice accelerated diffusion-weighted imaging with higher spatial resolution for patients with liver metastases from neuroendocrine tumours. Clinical Radiology 76, 81. e11-81. e19 (2021).
4. Inoue, Y. et al. Quantitative Evaluation of Display Contrast of Gd-EOB-DTPA-Enhanced Magnetic Resonance Images: Effects of the Flip Angle and Grayscale Gamma Value. Radiology research practice 2019 (2019).
5. Chakraborty, D. P. Recent advances in observer performance methodology: jackknife free-response ROC (JAFROC). Radiation protection dosimetry 114, 26-31 (2005).
6. Obele, C. C. et al. Simultaneous multislice accelerated free-breathing diffusion-weighted imaging of the liver at 3T. Abdominal imaging 40, 2323-2330 (2015).
7. Dietrich, O., Heiland, S. & Sartor, K. Noise correction for the exact determination of apparent diffusion coefficients at low SNR. Magnetic Resonance in Medicine: An Official Journal of the International Society for Magnetic Resonance in Medicine 45, 448-453 (2001).
Figures

Figure 1. Flowchart of the study population.
All 144 patients who underwent liver or pancreaticobiliary MR during a 3-month period was included for quantitative and qualitative analysis, while 67 focal lesions from 49 patients were included for focal lesion detectability analysis.
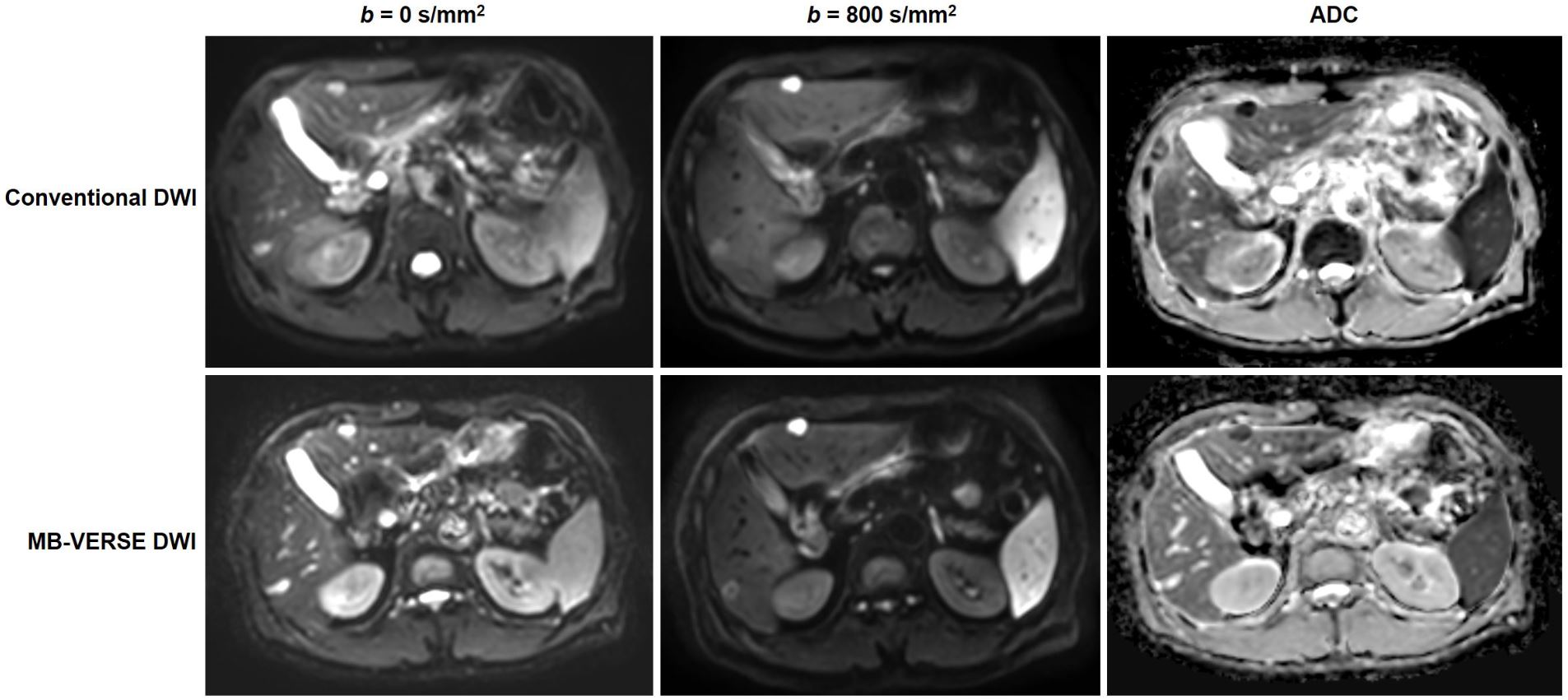
Figure 2. Diffusion-weighted image (DWI) and apparent diffusion coefficient (ADC) of a male patient with rectal cancer and liver metastasis.
The MB-VERSE DWI (SNR 52.1, CNR 190.4) showed lower SNR but higher CNR compared to those of the conventional DWI (SNR 87.3, CNR 172.6). ADC values (×10-3 mm2/s) of the liver and focal liver lesion was higher in the MB-VERSE DWI (liver, 1470.9; focal lesion 339.5) than those in the conventional DWI (liver 1087.0; focal lesion 100.6). The scan time for the MB-VERSE DWI was shorter than the conventional DWI (99.0 versus 129.3 seconds).
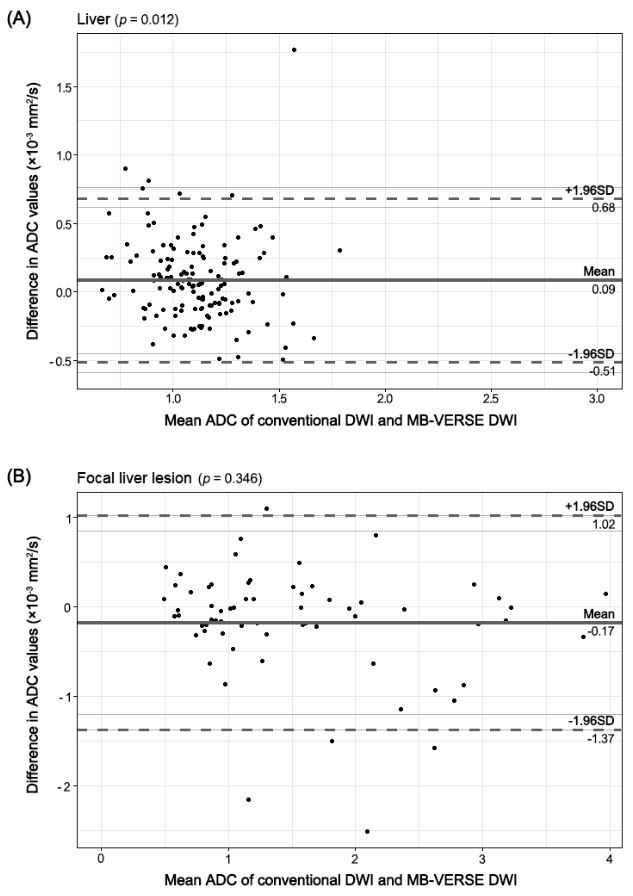
Figure 3. Bland-Altman plots to compare agreeability of ADC values between the conventional DWI and MB-VERSE DWI. (A) ADC values for the liver parenchyma was slightly higher than the those of the conventional DWI with statistical significance. (B) ADC values for focal liver lesions was not significantly different between the MB-VERSE DWI and the conventional DWI with virtually no bias. The p-values for Wilcoxon signed rank test is indicated on each panel.