2404
MRI of the Post-Operative Hip Following Arthroscopic Repair: What are the Imaging Characteristics of Labrum Re-Tear and Capsular Complications?1Radiology, University of Wisconsin School of Medicine and Public Health, Madison, WI, United States, 2Orthopedic Surgery, University of Wisconsin School of Medicine and Public Health, Madison, WI, United States
Synopsis
After acetabular labrum repair an intact repair, labrum re-tear, adhesions, and capsular disruption can have variable appearance on MRI. Some signs have been described as evidence of labral re-tear and adhesions. We retrospectively evaluated 25 hip MRIs in patients who later underwent revision arthroscopy utilizing these signs. Results were compared to arthroscopic findings. Fluid signal within the labrum demonstrated a high specificity for re-tear. Signs of adhesion were often identified accurately but could be imitated by synovitis. Capsular disruption was also identified with high sensitivity.
Introduction:
The torn acetabular labrum, often associated with femoroacetabular impingement syndrome (FAIS), is surgically treated with arthroscopy and labral repair. A repaired labrum can have variable appearances on magnetic resonance imaging (MRI), which makes differentiating reinjury versus expected post-operative changes very difficult. A handful of labrum morphologies have been proposed to aid in the diagnosis of re-tear. Additional post-operative changes including adhesions and capsular defects could also lead to recurrent/persistent pain after labral repair. Our goal was to further evaluate the proposed labrum morphologies in diagnosing labrum tear, signs of adhesion and capsular defects on MRI, and then compare these to arthroscopic findings of the torn labrum in those patients who undergo revision hip arthroscopy.Methods:
IRB approval was obtained to perform a retrospective review of arthrographic and non-arthrographic hip MR exams from 2018 - 2021 with a history of labral repair. All patients underwent subsequent revision arthroscopy by a single hip preservation fellowship-trained, board-certified orthopedic surgeon with a high-volume hip arthroscopy practice. Three readers (2 MSK radiologists and 1 MSK fellow), independently evaluated the MR studies blinded to the repeat arthroscopic findings. Six criteria were used to evaluate the labrum including presence of a paralabral cyst, labral enlargement, labral diminution, labral distortion, intrasubstance signal intensity (SI), and basal SI. The intrasubstance and basal SI were divided into dark, intermediate, and bright (fluid or near fluid SI). Presence of adhesions at the femoral neck, within the perilabral sulcus, or obliteration of the perilabral sulcus, and capsular defects were also recorded. Discrepancies between the independent results were resolved by consensus. Results were compared to the arthroscopic findings, determining the accuracy of the criteria to true labral tears and identifying adhesions and capsular defects.Results:
The study group consisted of 25 patients (19 women and 6 men) with a mean age of 32 years (17-55). There were 22 arthrographic studies and 3 non-arthrographic studies. 21/25 (84%) of the patients had a recurrent or new labrum tear on arthroscopy. 17/25(68%) were accurately diagnosed on MR, 1/25 (4%) was diagnosed with a tear at a different clockface and was categorized as a false positive, and 3/25 (12%) tears were not visualized on MR. No paralabral cysts were present. 6/25 (24%) labrum were enlarged, all of which correlated with tears (Accuracy 28% (Acc)). 17/25 (68%) labrum were diminutive, 13 of which correlated with tears (Acc 56%). 18/25 (72%) labra were distorted, 13 of which correlated with tears (Acc 52%). Intermediate intrasubstance SI was present in 15/25 (60%) labrum, 10 of which correlated with tears (Acc 50%). Bright intrasubstance SI was present in 5/25 (20%) labrum, all of which correlated with tears (Acc 52%, specificity 100%). Intermediate basal SI was present in 11(44%) labrum, 8 of which correlated with tears (Acc 67%). Bright basal SI was present in 13/25 (52%) labrum, 11 of which correlated with tears (Acc 56%). Only the 22 arthrographic studies were assessed for adhesions and capsular defects. 15 of the arthrograms were diagnosed with adhesions, 11 of which were confirmed on arthroscopy (Acc 59%), the other 4 correlated with significant synovitis. When accounting for both adhesions and/or significant synovitis accuracy rose to 77%. 7 exams were diagnosed with a capsular defect, 3 of which were present on arthroscopy (Acc 82%).Discussion:
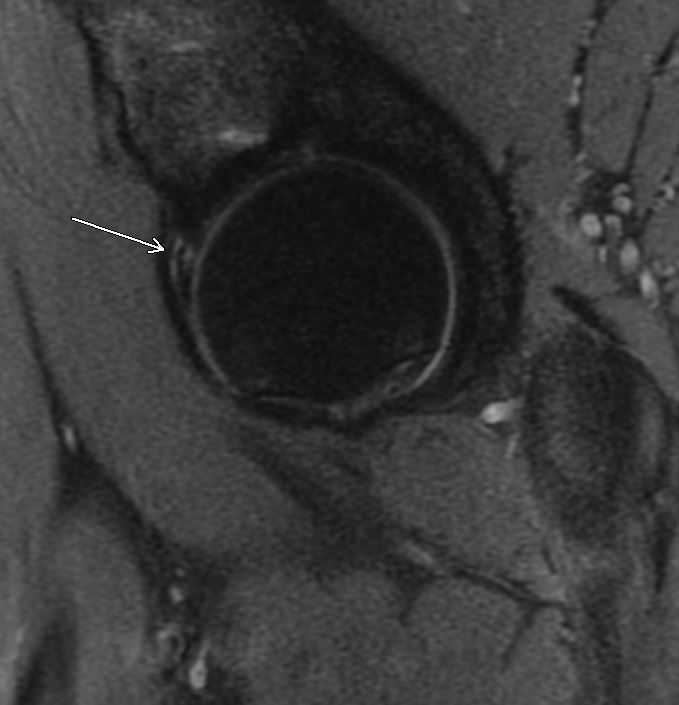
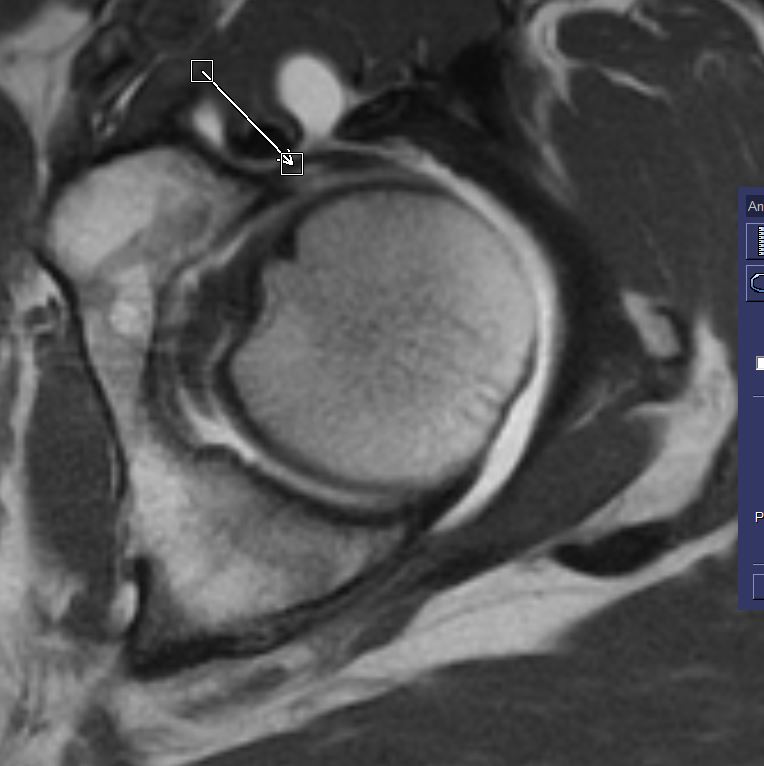
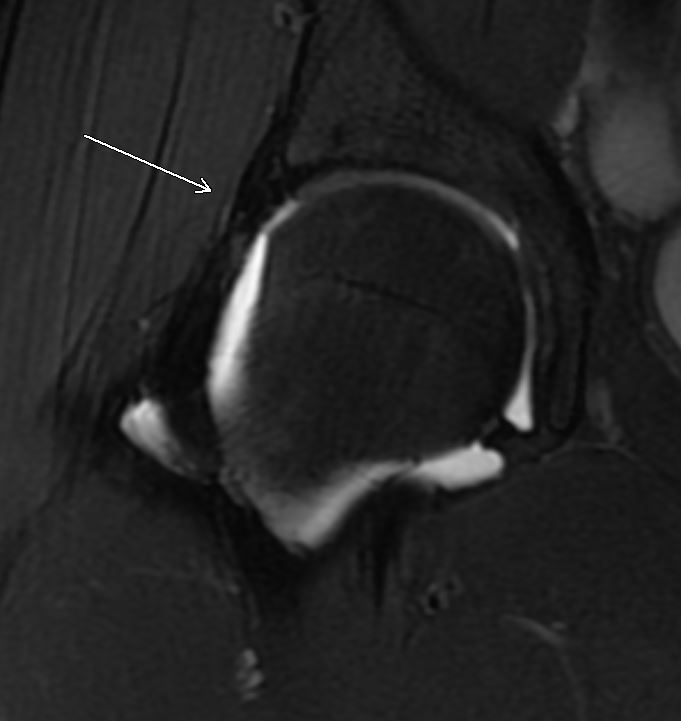
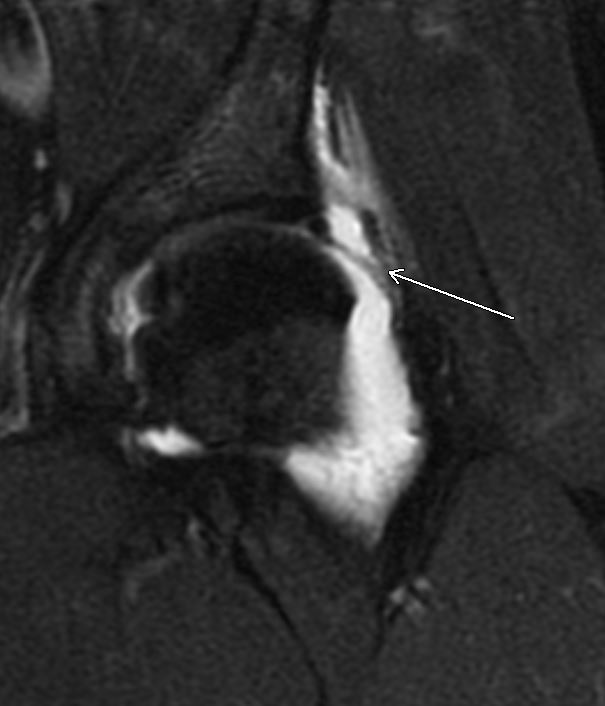
We utilized 6 criteria to evaluate the post-operative labrum. No paralabral cysts were present in our cohort. Of the remaining 5 criteria, all were more common in the reinjured labra. However, sensitivity and/or specificity for the criteria was moderate, low or unbalanced. Fluid or near fluid intrasubstance SI was not often present but demonstrated 100% specificity for labrum re-tear. This signal often, though not always seen to extended to the labral surface. Postoperative adhesions may be present in symptomatic and asymptomatic patients. We evaluated for adhesions and capsular disruption on the 22 arthrographic studies. 14 patients had greater than “minimal” adhesions on arthroscopy; 11 of the 14 (78%) were able to be diagnosed with MRI. There were 4 false positive adhesion diagnoses on MRI though all 4 had “significant synovitis” on arthroscopy which may have been a confounding factor leading to findings previously ascribed to adhesions such as an obliterated perilabral sulcus. Of the 4 patients who did not have a labral tear on repeat arthroscopy, 2 had severe capsulolabral adhesions (also diagnosed on MRI), 1 had ossification of the labrum, and 1 had an unstable hypertrophied labrum all of which were repaired. Sensitivity and exclusion of capsular defects was highly accurate, however it also resulted in a nearly equal number of false positives.Conclusion:
Our study showed that previously described MRI criteria for labral reinjury is more common in torn labrum compared to intact repairs. However, these signs currently lack the sensitivity and specificity to be fully reliable. Fluid or near fluid intrasubstance signal is not often seen but may be a more specific finding to suggest re-tear. Intraarticular adhesions which can be a source of pain, are often identified post operatively and may be mimicked by synovitis. Capsular disruption had good sensitivity with arthroscopic findings when suggested on MRI.Acknowledgements
No acknowledgement found.References
Samim M, Youm T, Burke C, Meislin R, Vigdorchik J, Gyftopoulos S. Hip arthroscopy-MRI correlation and differences for hip anatomy and pathology: What radiologists need to know. Clin Imaging. 2018 Nov-Dec;52:315-327.
Dietrich T. J., et al. Postoperative imaging in femoroacetabular impingement. Semin Musculoskelet Radiol. 2013 Jul; 17(3):272-8.
Aprato A., et al. The accuracy of magnetic resonance arthrography in hip arthroscopic labral revision surgery. Hip International 2013; 23(1):99-103.
Smith, T.O., Hilton, G., Toms, A.P. et al. The diagnostic accuracy of acetabular labral tears using magnetic resonance imaging and magnetic resonance arthrography: a meta-analysis. Eur Radiol 21, 863–874 (2011).
Haefeli PC, Schmaranzer F, Steppacher SD, Cullmann JL, Tannast M, Büchler L. Imaging appearance and distribution of intra-articular adhesions following open FAI surgery. Eur J Radiol. 2018 Jul;104:71-78.
Beck M. Groin pain after open FAI surgery: the role of intraarticular adhesions. Clin Orthop Relat Res. 2009 Mar;467(3):769-74.
Kim C. O., Dietrich T. J., et al. Arthroscopic Hip Surgery: Frequency of Postoperative MR Arthrographic Findings in Asymptomatic and Symptomatic Patients. Radiology 2017; 283(3):779-788
Figures