2347
Eliminating limits of spatiotemporal resolution in radial stack-of-stars imaging using FID navigators and single-readout binning1Radboud University Medical Centre, Nijmegen, Netherlands, 2German Cancer Research Center (DKFZ), Heidelberg, Germany, 3NYU Langone Medical Center, New York, NY, United States
Synopsis
Motion-compensated images can be created from motion-binned undersampled radial stack-of-stars data through compressed sensing and image registration. However, for long repetition times or for many partitions, the acquisition time for one radial projection with all phase-encode steps becomes too long to sample the motion via self-gating, which leads to motion artifacts. Therefore, we estimate motion from FID-navigators and perform binning on a single-readout level to gain higher spatiotemporal resolutions. Our methods are tested on a motion phantom and volunteer with gridding and motion-compensated reconstructions. Our results show accurate detection of the motion signal and reduced motion blur in reconstructions.
Introduction
MRI of the thorax is challenging, as respiratory motion can induce blurring or ghosting artifacts.1 Breath-holding limits acquisition times to approximately 15 s, precluding high spatial resolutions over large fields-of-view.Radial sampling schemes are inherently motion robust.2 Furthermore, if golden-angle reordering is used, radial MR data can be retrospectively gated into multiple motion states according to a motion signal.3 A common method to extract the motion signal is to collect the data near the k-space center for projections of the total signal in the imaged volume at every $$$\Delta t = N_p\,T_R$$$, where $$$N_p$$$ is the number of partitions and $$$T_R$$$ is the repetition time.3-6 According to the Nyquist criterion, the detectable respiratory frequency in this case is limited to $$$f_s = 1/(2\,N_p\,T_R)$$$. For longer $$$T_R$$$, or many partitions, the acquisition time for a full stack of partitions per radial projection becomes too long to faithfully sample the motion, leading to temporal aliasing and motion blur when binning k-space data into different motion states.
We lift this restriction by acquiring a short free-induction decay (FID) navigator at every $$$T_R$$$, allowing single-readout binning (SRB) of the data into motion states, resolving motion frequencies up to $$$1/(2\,T_R)$$$. We test our method on a motion phantom and a normal breathing volunteer, reconstructing the data with a non-uniform fast Fourier transform (NUFFT) and an adapted version of the 4D motion-compensated high-dimensional total variation (MoCo-HDTV) algorithm, which is a framework for joint reconstruction and motion estimation for undersampled radial data.6
Methods
We acquired data of a motion phantom (Quasar MRI 4D, Modus QA, London, Canada) and volunteer with a golden-angle radial stack-of-stars spoiled gradient echo sequence7 (Table 1) on a 3-T MR system (Prisma-Fit, Siemens Healthineers, Erlangen, Germany). The phantom contained a central oscillating gel-filled cylinder. Maximum peak-to-peak translation was set to 3 cm and the frequency of the breathing-like motion pattern was approximately 0.25 Hz. $$$T_R$$$ and $$$N_p$$$ were chosen such that spoke angle binning (SAB), which includes all phase-encode steps per spoke orientation, was expected to lead to inaccurate motion estimates. We sampled 32 FID acquisition points in 200 µs between excitation and phase-encoding gradient as a navigator. For each spoke angle, all partitions were sampled in random order before moving to the next angle to ensure a more evenly distributed number of readouts in each partition and respiratory phase (Fig. 1).Respiratory motion signals were extracted as the first principal components of principal component analyses of the FID navigators and of the nine central points of every gradient-echo readout.6 We calculated the correlation coefficients of the FID and gradient-echo motion signals with the reference signal of the phantom. We reconstructed the data both with NUFFTs and via an adapted version of the MoCo-HDTV algorithm.6
To compare SAB and SRB independent of the method of motion detection, we created reconstructions for SAB with the means of the FID navigators across the partitions as the motion signal, since $$$Δt$$$ was too long to detect respiratory motion from the k-space center.
Results and Discussion
The FID motion signal shows a clear correspondence to the motion pattern imposed on the phantom, indicating that the rigid motion during acquisition was accurately extracted from the FID navigators (Fig. 2). Meanwhile, the gradient-echo motion signal is clearly aliased (Fig. 2). Calculated correlation coefficients of the FID and gradient-echo motion signals with respect to the reference equaled 0.98 and 0.26, respectively.SRB resulted in reduced motion blur in NUFFT reconstructions of the phantom data, and in higher through-plane incoherence of undersampling artifacts, which may be advantageous for compressed sensing reconstructions (Fig. 3).8
Figure 3 also shows comparisons of the MoCo-HDTV reconstructions for the phantom data again at end-exhalation, which greatly reduce the level of undersampling artifacts, although at the cost of slight motion blur. However, SRB, in comparison to SAB, leads to an increase of the effective spatial resolution by reducing motion blur between slices. Using SRB combined with MoCo-HDTV reconstruction on in vivo data leads to a sharp depiction of anatomical structures in the thorax and abdomen at high spatial resolution (Fig. 4).
Conclusion
We showed first results for the acquisition and reconstruction of radial stack-of-stars data where the temporal resolutions for motion detection and reconstruction are increased through FID navigators and single-readout binning. Images of a moving phantom and a volunteer show reduced motion blur, and more incoherent and less prominent streaking artifacts, allowing the detection of small anatomical structures in the upper abdomen in a free-breathing acquisition.Acknowledgements
We thank C. Schneider and U. Van der Heide of the Netherlands Cancer Institute (NKI) for providing the Quasar phantom.References
- Axel L, Summers RM, Kressel HY, et al. Respiratory effects in two-dimensional Fourier transform imaging. Radiology. 1986; 160:795-801.
- Glover GH, Pauly JM. Projection reconstruction techniques for reduction of motion effects in MRI. Magn Reson Med. 1992; 28(2):275-89.
- Feng L, Axel L, Chandarana H, et al. XD-GRASP: Golden-angle radial MRI with reconstruction of extra motion-state dimensions using compressed sensing. Magn Res Med. 2016; 75(2):775-88.
- Spincemaille P, Liu J, Nguyen T. Z-intensity-weighted position self-respiratory gating method for free-breathing 3D cardiac CINE imaging. Magn Reson Imaging. 2011; 29(6):861-8.
- Schneider M, Benkert T, Solomon E, et al. Free-breathing fat and R2*-quantification in the liver using a stack-of-stars multi-echo acquisition with respiratory-resolved model-based reconstruction. Magn Reson Med. 2020; 84(5): 2592-2605.
- Rank CM, Heußer T, Buzan MTA, et al. 4D respiratory motion-compensated image reconstruction of free-breathing radial MR data with very high undersampling. Magn Res Med. 2016; 77(3):0740-3194.
- Block, KT, Uecker, M. and Frahm, J. Undersampled radial MRI with multiple coils. Iterative image reconstruction using a total variation constraint. Magn. Reson. Med. 2007; 57:1086-1098.
- Lustig M, Donoho D, Pauly JM. Sparse MRI: the application of compressed sensing for rapid MR imaging. Magn Reson Med. 2007; 58(6):1182-1195.
Figures
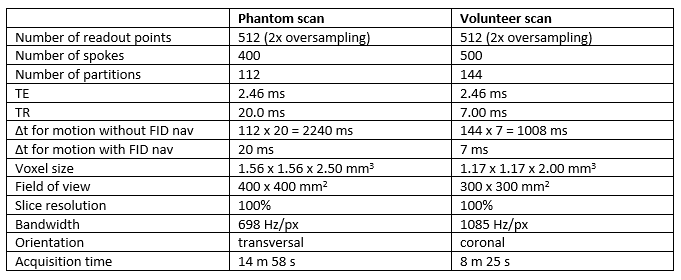
Table 1. Sequence parameters of the MR acquisitions of phantom and volunteer data. Δt for motion indicates the time interval between motion signal samples.
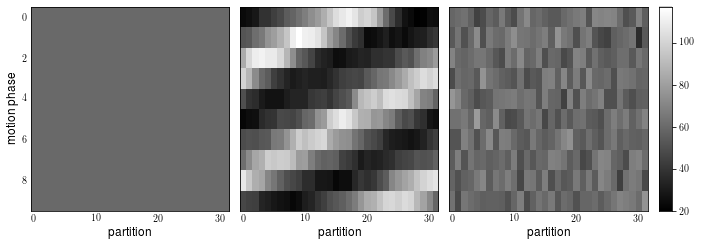
Figure 1. Distribution of the number of readouts per motion phase (for 10 unique phases) and partition for three different acquisition schemes: SAB (left), SRB with linear kz-reordering (center) and random kz-reordering (right). We suppress the periodicity in the distribution (center) by sampling partitions in random order (right).
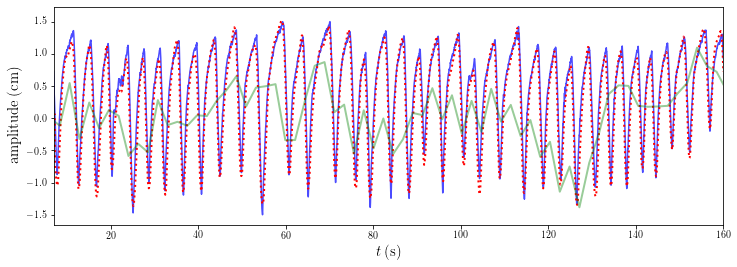
Figure 2. The phantom’s reference signal (blue line), the free-induction decay navigator signal (red dotted line) and the gradient-echo signal (green line). There is a clear correspondence between the reference and the FID-navigators (correlation coefficient of 0.98 with reference), apart from some under- or overestimation of motion in the end-inhalation phase. The gradient-echo signal is clearly aliased (correlation coefficient of 0.26 with reference).
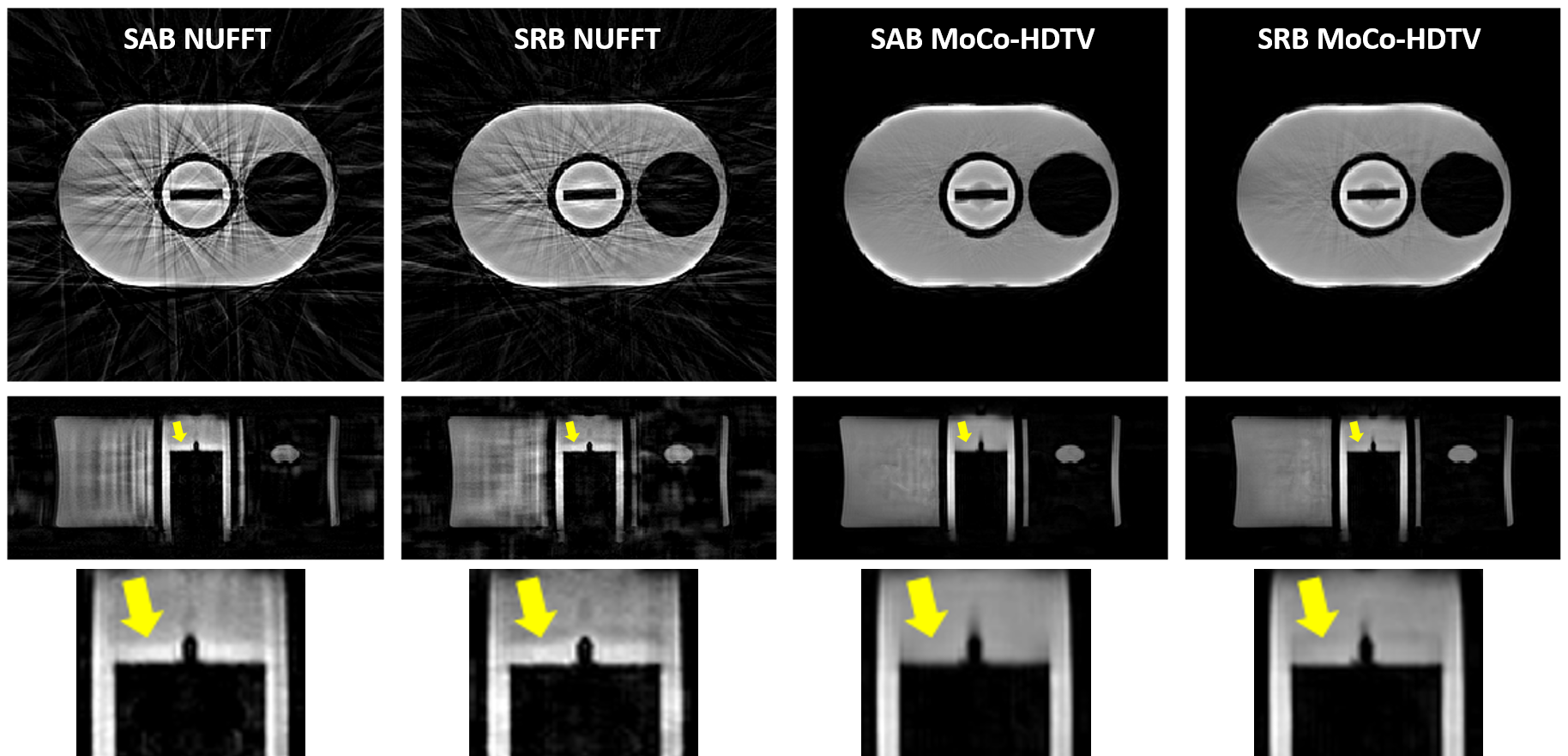
Figure 3. NUFFT and MoCo-HDTV reconstructions of the phantom data at end-exhalation with both the SAB and SRB methods. Images in the top row correspond to reconstructions in the readout plane. For images in the middle and bottom rows, the vertical axes of images correspond to the phase-encoding directions. The bottom row is a zoomed-in view of the oscillating cylinder's edge. SRB reduces the motion blur (arrows) and increases through-plane incoherence of the radial streak artifacts.

Figure 4. Transversal and coronal MoCo-HDTV reconstructions of the volunteer data with SRB. Data was acquired in coronal orientation. Contours of the diaphragm and liver are sharply delineated in both images.