2309
Feasibility of Simultaneous Bilateral Hip Quantitative MRI
Koren Roach1, Misung Han1, Thomas Link1, Richard Souza1, Sharmila Majumdar1, and Valentina Pedoia1
1UCSF, San Francisco, CA, United States
1UCSF, San Francisco, CA, United States
Synopsis
Our group recently developed simultaneous bilateral hip MR acquisition methods to reduce total imaging time and employ during longitudinal evaluations of hip OA. This study evaluated the ability of simultaneous bilateral 3D FSE Cube and MAPSS acquisitions to maintain relevant morphological information compared to unilateral acquisitions. The mean T1ρ and T2 values of the simultaneous bilateral MAPSS acquisitions were not significantly different from unilateral acquisitions and relaxometry map patterns were preserved. Additionally, our simultaneous bilateral hip protocol promoted high resolution 3D Cube images for morphological abnormality detection and reduced scan time by 40%, to under 30 minutes.
Introduction
Osteoarthritis (OA) is the primary cause of disability in the US,1 with hip OA afflicting up to 27% of adults over the age of 45.2 Biochemical changes in articular cartilage can be measured via magnetic resonance (MR) T1ρ and T2 relaxation times and coincide with or precede the development of OA.3 In cartilage, increased T1ρ corresponds to decreased proteoglycan content, while longer T2 relaxation times indicate increased water content and matrix disorganization, respectively.4, 5 To effectively study the progression of hip OA, both hips need to be evaluated and longitudinal studies must span several years and require acquisition on multiple scanners to stay current with technology. The aim of this work was to 1) evaluate the feasibility employing simultaneous bilateral hip imaging methods, and 2) compare images acquired with different scanner and coil configurations.Methods
Our hip imaging protocol included sagittally-combined T1ρ/T2 quantification sequences (Magnetization-Prepared Angle-Modulated Partitioned k-Space Spoiled Gradient Echo Snapshots (MAPSS))6 and three‐dimensional (3D) fast spin‐echo Cube sequences. A simultaneous bilateral hip imaging protocol and a unilateral hip imaging protocol were tested on a GE Signa Premier 3T MR scanner (GE Healthcare, Waukesha, WI; Scanner 1) having a maximum gradient amplitude of 7 G/cm and a maximum slew rate of 150 mT/m/ms. The imaging parameters and resolution from an established protocol on a Discovery MR750 3T scanner7 (GE Healthcare, Waukesha, WI, maximum gradient amplitude: 5 G/cm, maximum slew rate: 200 mT/m/ms; Scanner 2) were maintained (Tables 1-2). Three volunteers (3 female) were recruited and imaged on Scanner 1 and Scanner 2. On Scanner 1, each hip was imaged with a unilateral protocol and a simultaneous bilateral protocol, using a 30-channel adaptive image receive (AIR) anterior array coil and a spine posterior-array coil embedded into the table (GE Healthcare, Waukesha, WI). For bilateral acquisitions, shim volumes were located on each hip to provide more uniform B0/B1 fields over the joints, rather than the medial abdominal region. On Scanner 2, each hip was imaged unilaterally, using a 32-channel phased-array cardiac coil (Invivo Corp., Amsterdam, Netherlands) positioned over the hip of interest. The MAPSS images were fit with different TSL and TE values to calculate T1ρ and T2 relaxometry maps, respectively.6 Acetabular and femoral cartilage volumes were segmented on the MAPSS images (MatLab 2015b, The MathWorks, Natick, MA). Mean T1ρ and T2 values were calculated for the right and left acetabular and femoral cartilage volumes of each volunteer.8 Mixed repeated measures ANOVAs were performed to evaluate the effects of cartilage volume and MAPSS configuration (e.g., Scanner 1 simultaneous bilateral) on mean T1ρ and T2 values. Post-hoc pairwise tests with Bonferroni adjustments were performed if interactions were significant (R Development Core Team, v 4.0.3). Given that mean comparisons encompass large quantities of voxels across a cartilage volume, the relaxometry maps were visualized to assess if T1ρ and T2 voxel-wise patterns were preserved. The Cube sequences were qualitatively evaluated by a board-certified musculoskeletal radiologist (TML) to confirm image quality and spatial resolution sufficient for detecting abnormalities.Results
Simultaneous bilateral acquisitions reduced MAPSS scan time by 28.41% (Table 1) and Cube scan time by 50.72% (Table 2), for a total time reduction of 39.81%, compared to two sequential unilateral hip acquisitions. Significant interactions were found between MAPSS configurations (p = 0.006) and between cartilage volumes (p = 0.03) for left T2 values. However, pairwise tests revealed no significant interactions between cartilage volumes (p > 0.147) or protocol configurations (p > 0.135) after Bonferroni adjustment. There were no significant interactions for mean T1ρ values (p > 0.063) or right T2 values (p > 0.065). Qualitative analysis of T1ρ (Figure 1) and T2 (Figure 2) maps demonstrated good preservation of relaxometry patterns across the cartilage. A small labral tear and degenerative labral changes were identified on the Scanner 1 simultaneous bilateral Cube images, demonstrating no loss of the 3D resolution necessary to visualize morphological abnormalities compared to unilateral Cube sequences (Figure 3).Discussion
This feasibility study demonstrated the ability to acquire simultaneous bilateral hip images on Scanner 1, with a 40% reduction in scan time and without the need to reposition the coil between scans. The AIR coil array can cover both hips sufficiently for simultaneous imaging, and no significant decrease in SNR was observed by applying acceleration along the slab direction. Our simultaneous bilateral hip MAPSS acquisition retained quantitative accuracy within the cartilage volume and preserved voxel-wise patterns in the T1ρ and T2 relaxometry maps, which may suggest that B0/B1 field variations are not notably different between bilateral and unilateral acquisitions. Additionally, our simultaneous bilateral Cube acquisition demonstrated no detectable decrease in SNR and maintained visibility to morphological abnormalities, even in the reformatted images.Conclusion
Our simultaneous bilateral hip protocol preserved cartilage relaxometry values and patterns, which will promote consistency between scanner configurations over long-term studies. By reducing bilateral hip scan time from 45 minutes to under 30 minutes and eliminating the time required to switch coils from one hip to the other, these simultaneous bilateral hip protocols could be promising OA screening tools. Furthermore, the ability to compare both hips within the same image may be particularly useful for patients with unilateral hip OA.Acknowledgements
We would like to thank the volunteers for their time. This project was supported by NIH-NIAMS K24 AR072133 and NIH-NIAMS R01-AR069006.References
- C. f. D. Control and U. Prevention, Prevalence and most common causes of disability among adults--United States, 2005, MMWR: Morbidity and mortality weekly report, 2009, 58(16), 421-426, doi:
- J. M. Jordan, C. G. Helmick, J. B. Renner, G. Luta, A. D. Dragomir, J. Woodard, F. Fang, T. A. Schwartz, A. E. Nelson, L. M. Abbate, L. F. Callahan, W. D. Kalsbeek, and M. C. Hochberg, Prevalence of hip symptoms and radiographic and symptomatic hip osteoarthritis in African Americans and Caucasians: the Johnston County Osteoarthritis Project, J Rheumatol, 2009, 36(4), 809-815, doi: 10.3899/jrheum.080677.
- V. Pedoia, C. Russell, A. Randolph, X. Li, S. Majumdar, and A.-A. Consortium, Principal component analysis-T1rho voxel based relaxometry of the articular cartilage: a comparison of biochemical patterns in osteoarthritis and anterior cruciate ligament subjects, Quant Imaging Med Surg, 2016, 6(6), 623-633, doi: 10.21037/qims.2016.11.03.
- U. Duvvuri, R. Reddy, S. D. Patel, J. H. Kaufman, J. B. Kneeland, and J. S. Leigh, T1rho-relaxation in articular cartilage: effects of enzymatic degradation, Magn Reson Med, 1997, 38(6), 863-867, doi:
- M. T. Nieminen, J. Rieppo, J. Toyras, J. M. Hakumaki, J. Silvennoinen, M. M. Hyttinen, H. J. Helminen, and J. S. Jurvelin, T2 relaxation reveals spatial collagen architecture in articular cartilage: a comparative quantitative MRI and polarized light microscopic study, Magn Reson Med, 2001, 46(3), 487-493, doi: 10.1002/mrm.1218.
- X. Li, C. Wyatt, J. Rivoire, E. Han, W. Chen, J. Schooler, F. Liang, K. Shet, R. Souza, and S. Majumdar, Simultaneous acquisition of T1rho and T2 quantification in knee cartilage: repeatability and diurnal variation, J Magn Reson Imaging, 2014, 39(5), 1287-1293, doi: 10.1002/jmri.24253.
- K. E. Roach, V. Pedoia, J. J. Lee, T. Popovic, T. M. Link, S. Majumdar, and R. B. Souza, Multivariate functional principal component analysis identifies waveform features of gait biomechanics related to early-to-moderate hip osteoarthritis, J Orthop Res, 2021, 39(8), 1722-1731, doi: 10.1002/jor.24901.
- V. Pedoia, X. Li, F. Su, N. Calixto, and S. Majumdar, Fully automatic analysis of the knee articular cartilage T1rho relaxation time using voxel-based relaxometry, J Magn Reson Imaging, 2016, 43(4), 970-980, doi: 10.1002/jmri.25065.
Figures
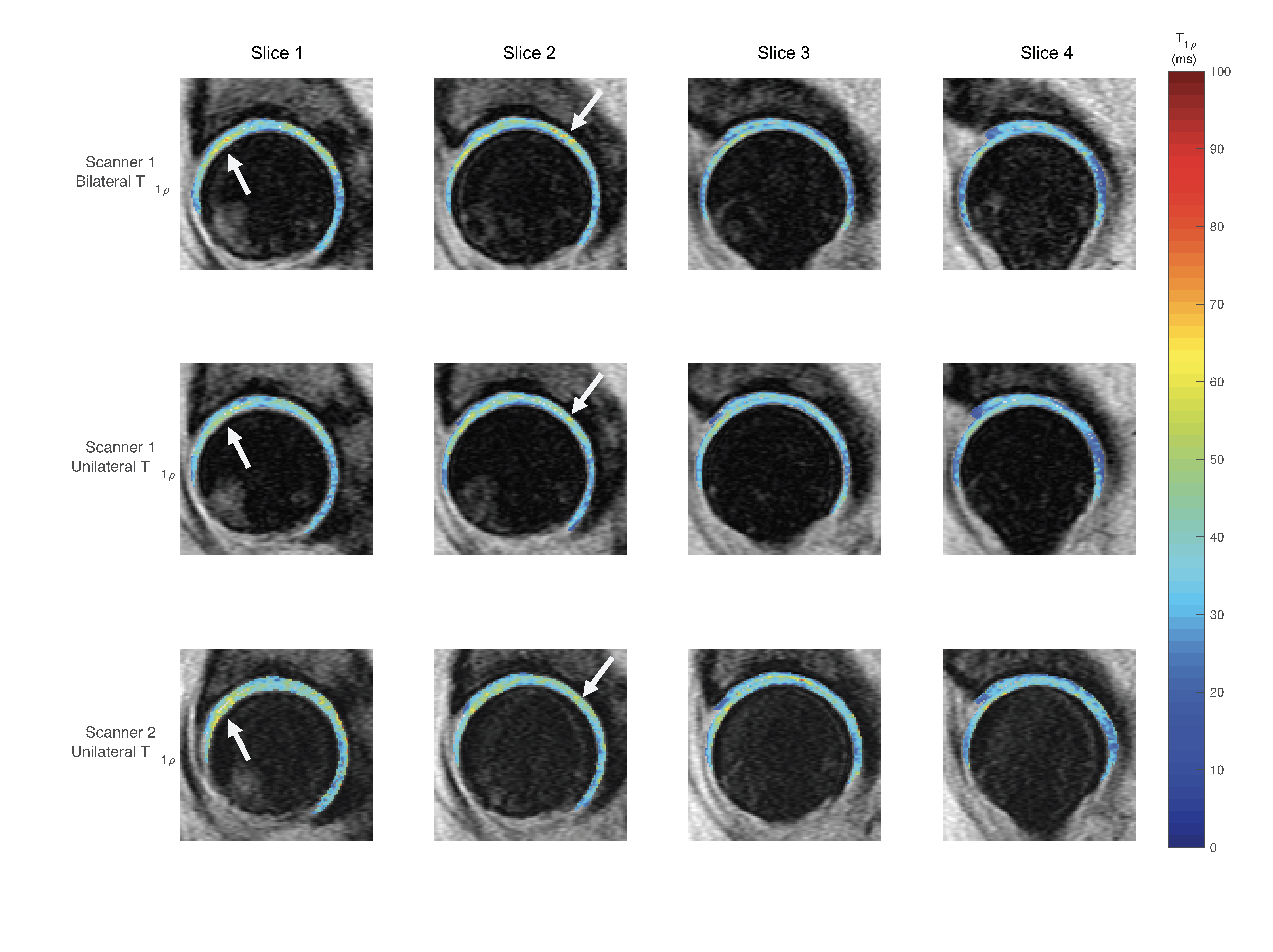
Figure 1: Scanner 1 simultaneous bilateral (top row), Scanner 1 unilateral (middle row), and Scanner 2 unilateral (bottom row)acetabular and femoral cartilage T1ρ relaxometry maps of one volunteer. Mean T1ρ values were not significantly different between sequence configurations and patterns across the pixels were preserved (indicated by arrows).

Figure 2: Scanner 1 simultaneous bilateral (top row), Scanner 1 unilateral (middle row), and Scanner 2 unilateral (bottom row)acetabular and femoral cartilage T2 relaxometry maps of one volunteer. Mean T2 values were not significantly different between sequence configurations and patterns across the pixels were preserved (indicated by arrows).
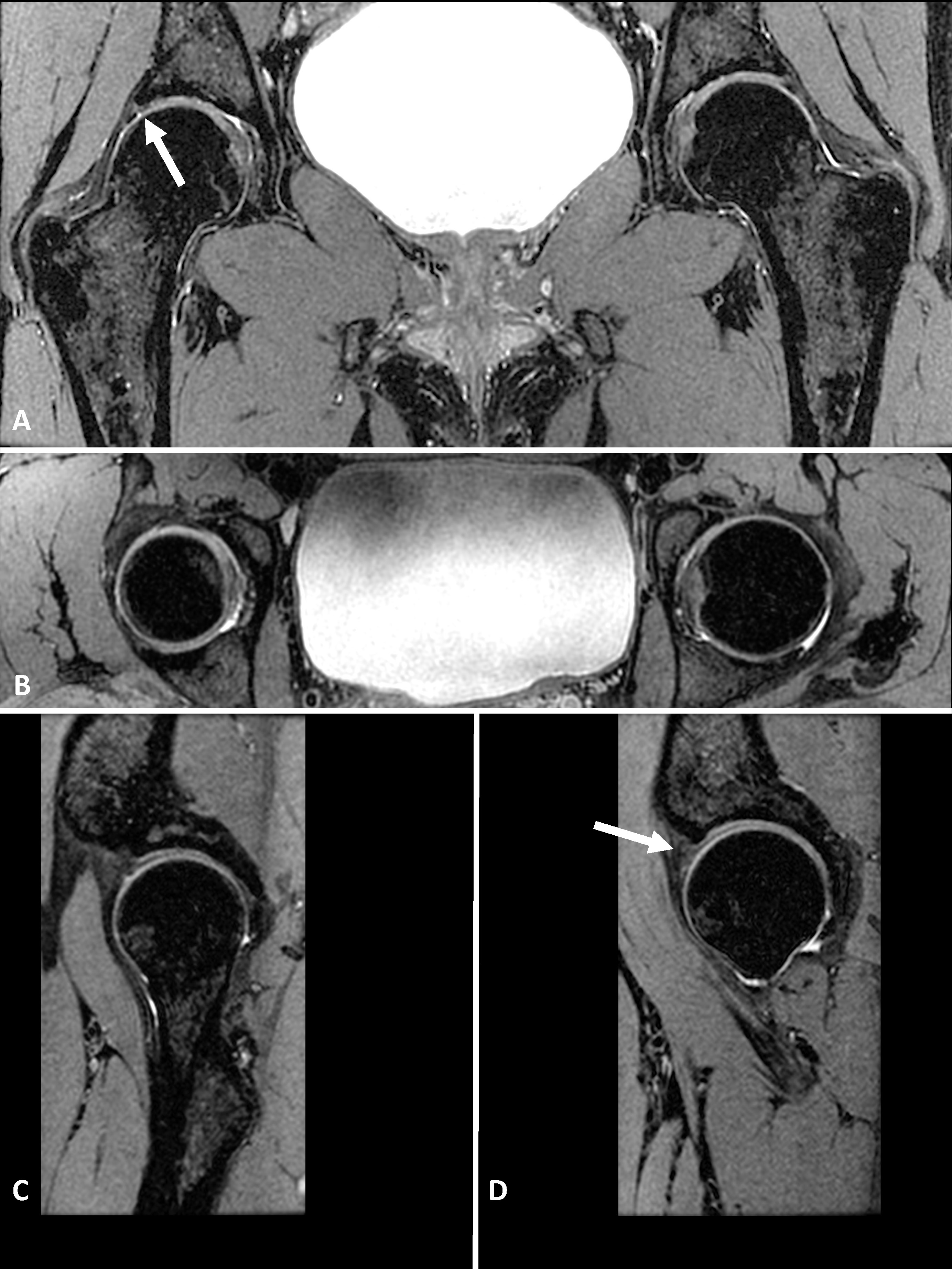
Figure 3: Simultaneous bilateral hip coronal acquisition of three‐dimensional (3D) fast spin‐echo Cube images of one volunteer. Visibility to morphological features of the hip joint cartilage and capsule were preserved. A) Coronally-acquired bilateral hip images, with an arrow indicating a small labral tear; B) axial reformat of simultaneous bilateral hips; C) and D) are sagittal reformats of the right and left hip, respectively, with an arrow (D) demonstrating the location of degenerative labral changes.
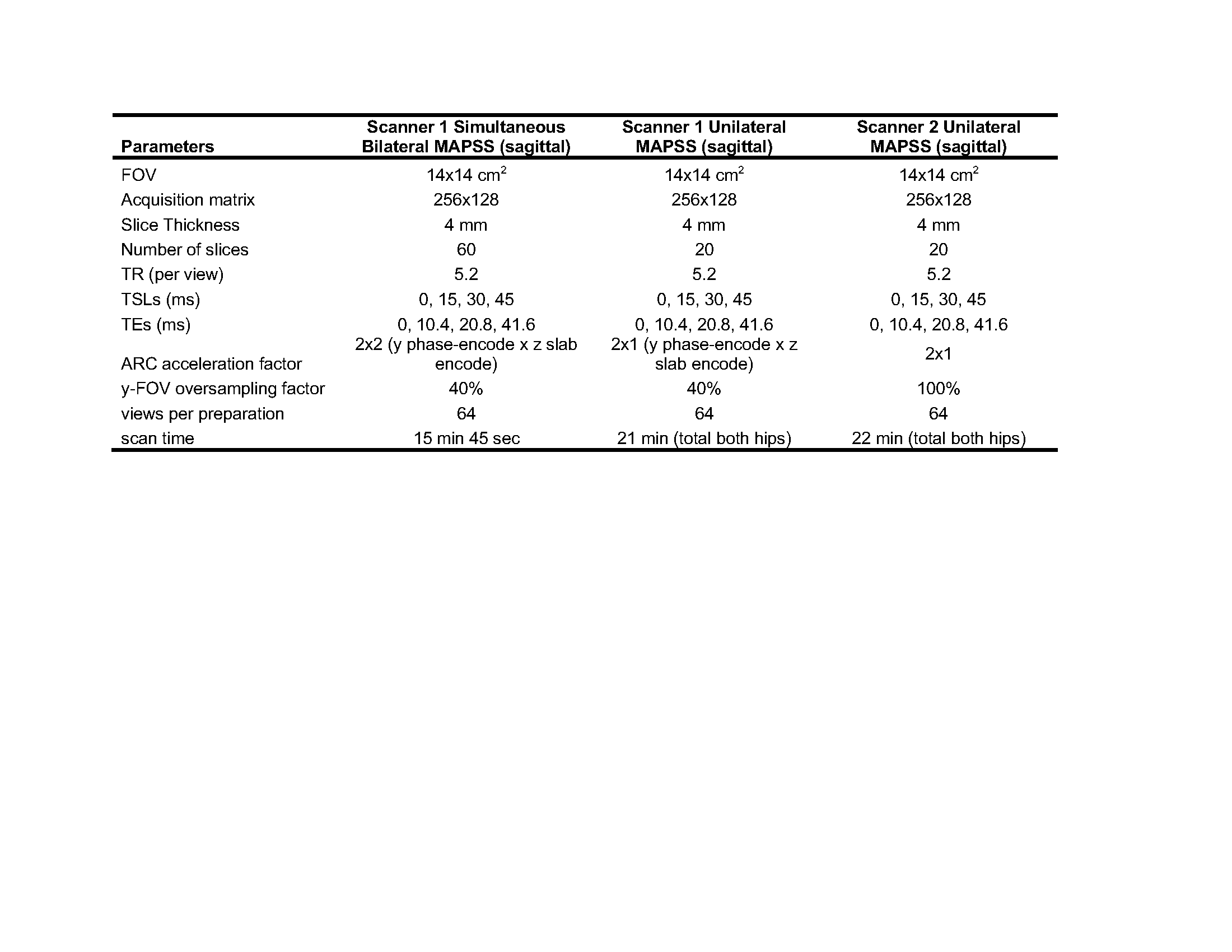
Table 1: Magnetic resonance (MR) Magnetization-Prepared Angle-Modulated Partitioned k-Space Spoiled Gradient Echo Snapshots (MAPSS) acquisition parameters.
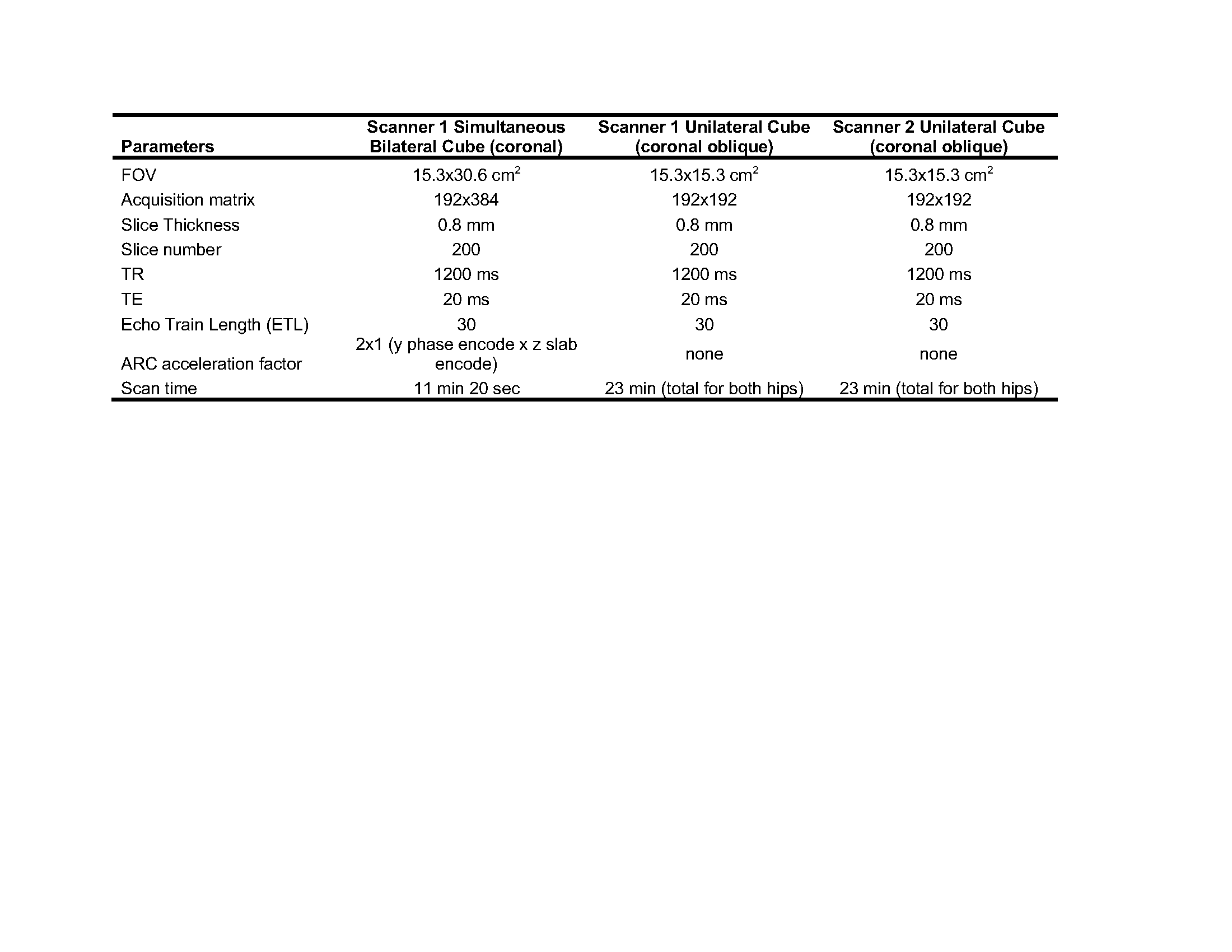
Table 2: Magnetic resonance (MR) 3D fast spin‐echo Cube acquisition parameters.
DOI: https://doi.org/10.58530/2022/2309