2299
Analysis of knee joint injury caused by training of freshmen based on 3T MRI and Automatic Cartilage Segmentation Technology :A prospective study1Department of Radiology, First Affiliated Hospital of Army Medical University, chongqing, China, 2Department of nuclear medicine, First Affiliated Hospital of Army Medical University, chongqing, China, 3First Affiliated Hospital of Army Medical University, chongqing, China, 4Siemens Healthineers Ltd., shanghai, China, 5MR Application Predevelopment, Siemens Healthcare GmbH, Erlangen, Germany, 6Health Service Training Base of the Army Military Medical University., chongqing, China, 7Health Service Training Base of the Army Military Medical University, chongqing, China
Synopsis
Magnetic resonance imaging (MRI) is the preferred choice for evaluating knee joint injury, which commonly occurs during physical training. In this study, we compared the effects of long-walking and regular daily training on knee joint injuries and cartilage microstructure in 23 young freshmen by analyzing 3D-DESSWE and T2 mapping images using the automatic cartilage segmentation prototype software. Our results demonstrated that regular daily training strengthens the knee joints and protects against knee joint injury by increasing the volume of the knee cartilage. Moreover, knee joint injury caused by short-term long walking and high-intensity pull training was reversible.
Introduction
Improper physical training can cause serious and irreversible damage to the knee joint. Magnetic resonance imaging (MRI) is the most effective and noninvasive method to diagnose or evaluate knee joint injury, which is very common during physical training [1-4]. MRI is generally used to precisely analyze morphological and biochemical changes in the knee cartilage [3, 5-7]. However, differential effects of various exercises on knee joint injury have not been well documented. In this study, we compared the effects of long-walking and regular daily physical training on acute and chronic knee joint injuries as well as cartilage microstructure by analyzing 3D-DESS and T2 mapping images using the automatic cartilage segmentation prototype software.Methods
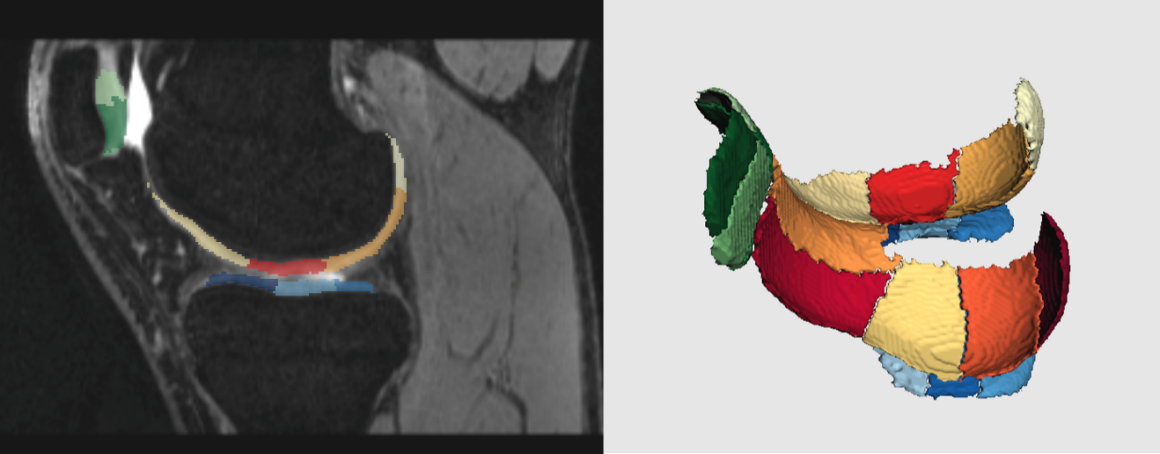
We recruited 23 young male college freshmen to participate in an 8-day 240 km long distance walk at an altitude of 168 ~ 400 meters (Table 1). The participant data was divided into the following three groups: before training (baseline group); 1 day after long-walking (long-walking group), and one year after daily physical training (Daily training group). We performed three-dimensional dual echo steady state with water excitation (3D-DESSWE), 2D T2 mapping, DIXON, T2WI and T1WI of the right knee joint using the MAGNETOM Trio 3T MR scanner (Siemens Healthcare, Erlangen, Germany) [8]. The automatic cartilage segmentation prototype software (MR Chondral Health version 2.1, Siemens Healthcare, Erlangen, Germany) [8] was used to automatically estimate cartilage volume, cartilage thickness, and T2 values of 21 subregions of the knee cartilage from the 3D-DESSWE and 2D T2 mapping images (Figure 1). We then graded the meniscus and cartilage damage (5-point system), bone marrow edema, ligament injury, and joint effusion (3-point system) [9-12]. Friedman’s test and Wilcoxon paired rank-sum test were used to compare the quantitative indices of knee cartilage in the baseline, long-walking, and daily training groups.Results
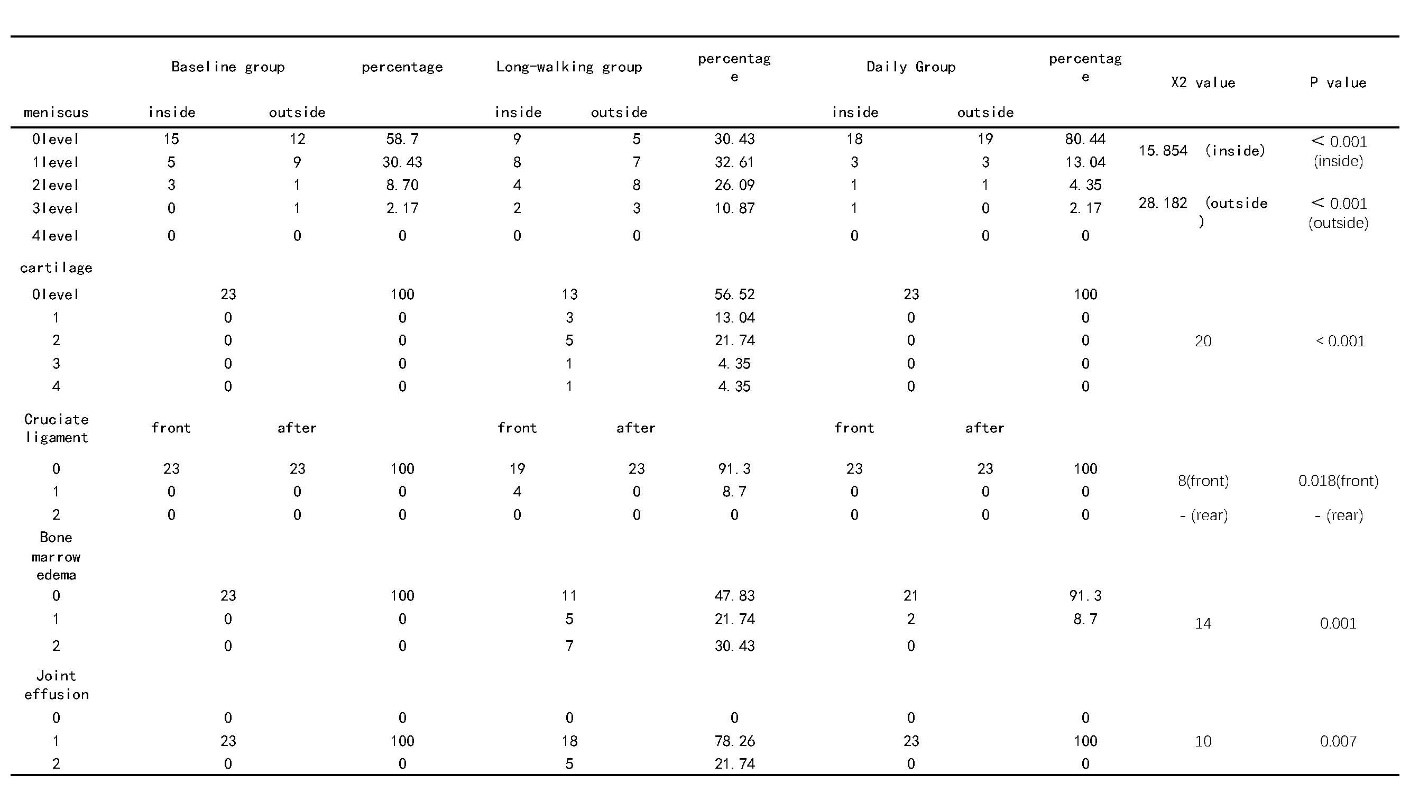
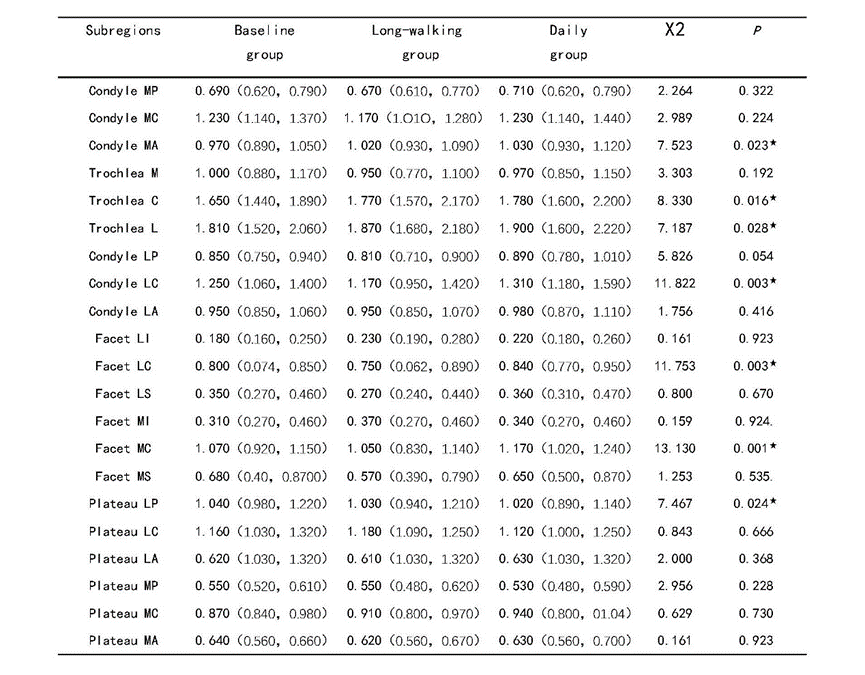
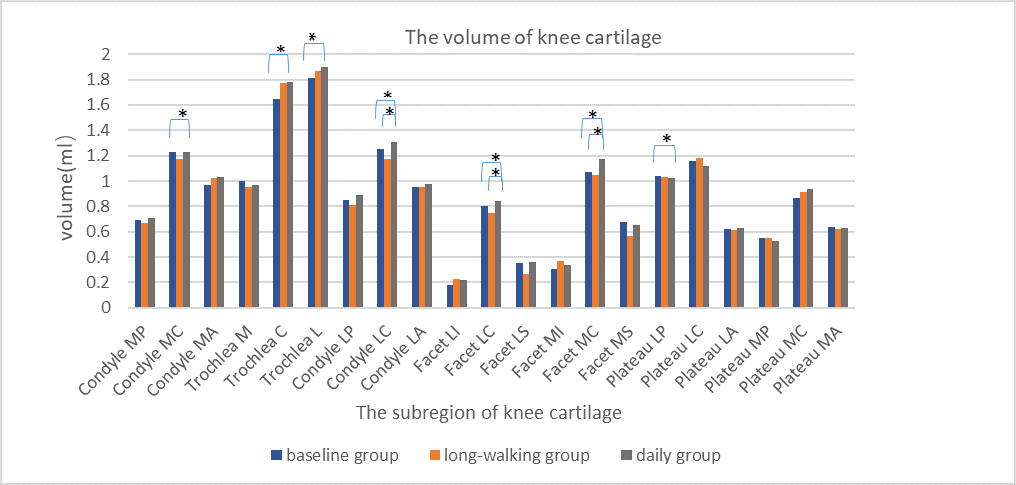
The injury to the medial meniscus and anterior cruciate ligament of the knee joint, joint effusion and bone marrow edema was significantly higher in the long-walking group compared to the baseline and daily training groups (Table 2). Furthermore, injury to the lateral meniscus was significantly worse in the long-walking group compared to the baseline group, but was significantly better in the daily training group compared to the baseline group (Table 2). We did not observe any significant changes to the posterior cruciate ligament among all the three groups (Table 2). The volume of knee cartilage was significantly increased, mainly in the stress surface of the femur, patella, and the lateral area of tibial plateau (trochlea C, trochlea L, condyle Ma, condyle LC, facet MC and facet LC). However, regular daily training did not significantly change thickness of the knee cartilage. Conversely, thickness of the knee cartilage decreased in the long-walking group, especially in the medial and lateral areas of femur and tibial plateau (condyle MP, condyle LP, condyle MC, facet LC, facet MC, plateau LP, plateau LC, plateau La, plateau MP and plateau MC) (Table 3, Figure 2). Moreover, significant changes were not observed in the knee cartilage volume of the long-walking group (Table 3, Figure 2). Both long-walking and daily training groups showed reduced T2 values of the knee joint compared to the baseline.Discussion & Conclusion
The muscle strength of the baseline group subjects was weak without regular systematic exercise. We demonstrated that long-walking training resulted in high load torsion, tension, and compression of the knee joint. This damaged the knee meniscus and the anterior cruciate ligament, and increased bone marrow edema, and joint effusion. Horga et al reported sustained improvements in the bone marrow and articular cartilage lesions of novice marathon runners [13]. Daily training significantly increased knee cartilage volume, mainly in the stress surface of femur, patella and the lateral area of tibial plateau, but thickness of the knee cartilage did not change. Lu and Wang reported that knee cartilage volume showed significant reduction in young adults after 12-weeks of running and cycling, but did not show any significant change after non-impact swimming and low-impact power striding [14]. Moreover, long walking and regular daily training decreased T2 signal intensity of the knee joint. Karanfil et al reported that 30 minutes of running exercise decreased T2 signal intensity of the knee joint cartilage without affecting its thickness [15]. In conclusion, our results show that regular daily training does not cause any serious injury to the knee joint, but strengthens the knee joint by increasing volume of the knee cartilage. Moreover, knee cartilage injury caused by short-term long walking was reversible.Acknowledgements
We sincerely thank all the study participants.
References
1. Leiter JRS, MacDonald L et al. Intrinsic stresses on bone and cartilage in the normal and anterior cruciate ligament-reconstructed knee before and after a half marathon: a magnetic resonance imaging analysis. Clin J Sport Med. 2012; 22(5):439-442.
2. Qiu L, Perez J, Emerson C, Barrera CM, Zhong J, Nham F, et al. Biochemical changes in knee articular cartilage of novice half-marathon runners. J Int Med Res. 2019; 47(11):5671-5679.
3. Schutz U, Ehrhardt M, God S, Billich C, Beer M, Trattnig S. A mobile MRI field study of the biochemical cartilage reaction of the knee joint during a 4,486 km transcontinental multistage ultra-marathon using T2* mapping. Sci Rep. 2020; 10(1):8157.
4. Zhang Y, Shu D, Yao W, Ding J, Chen L, Lin X, et al. MRI study of changes in knee bone marrow edema-like signal in asymptomatic amateur marathon runners before and after half-marathon running. Clin Imaging. 2021; 80:150-157.
5. Glaser C, Faber S, Eckstein F, Fischer H, Springer V, Heudorfer L, et al. Optimization and validation of a rapid high-resolution T1-w 3D FLASH water excitation MRI sequence for the quantitative assessment of articular cartilage volume and thickness. Magn Reson Imaging. 2001; 19(2):177-185.
6. Graichen H, Jakob J, von Eisenhart-Rothe R, Englmeier KH, Reiser M, Eckstein F. Validation of cartilage volume and thickness measurements in the human shoulder with quantitative magnetic resonance imaging. Osteoarthritis Cartilage. 2003; 11(7):475-482.
7. Wang Z, Ai S, Tian F, Liow MHL, Wang S, Zhao J, et al. Higher Body Mass Index Is Associated With Biochemical Changes in Knee Articular Cartilage After Marathon Running: A Quantitative T2-Relaxation MRI Study. Orthop J Sports Med. 2020; 8(8):2325967120943874.
8. Fripp J, Crozier S, Warfield SK, Ourselin S. Automatic segmentation and quantitative analysis of the articular cartilages from magnetic resonance images of the knee. IEEE Trans Med Imaging. 2010; 29(1):55-64.
9. Kocabey Y TO, Isbell W M , et al. The value of clinical examination versus magnetic resonance imaging in the diagnosis of meniscal tears and anterior cruciate ligament rupture. Arthroscopy 2004; 20(7):696-700.
10. Outerbridge R. The etiology of chondromalacia patellae. 43-B:752-757. J Bone Joint Surg. 1961; 43-B (4):752-757.
11. Link TM VV, Stehling C, et al. High-resolution MRI vs multislice spiral CT: Which technique depicts the trabecular bone structure best? European Radiology. 2003; 13(4):663-671.
12. Schueller-Weidekamm C, Schueller G, Uffmann M, Bader TR. Does marathon running cause acute lesions of the knee? Evaluation with magnetic resonance imaging. Eur Radiol. 2006; 16(10):2179-2185.
13. Horga LM, Henckel J, Fotiadou A, Hirschmann AC, Di Laura A, Torlasco C, et al. Is the immediate effect of marathon running on novice runners' knee joints sustained within 6 months after the run? A follow-up 3.0 T MRI study. Skeletal Radiol. 2020; 49(8):1221-1229.
14. Yubin LLaW. Effects of exercises on knee cartilage volume in young healthy adults: a randomized controlled trial. Chin Med J. 2014:127 (12): 2316-2321.
15. Karanfil Y, Babayeva N, Donmez G, Diren HB, Eryilmaz M, Doral MN, et al. Thirty Minutes of Running Exercise Decreases T2 Signal Intensity but Not Thickness of the Knee Joint Cartilage: A 3.0-T Magnetic Resonance Imaging Study. Cartilage. 2019; 10(4):444-450.
Figures
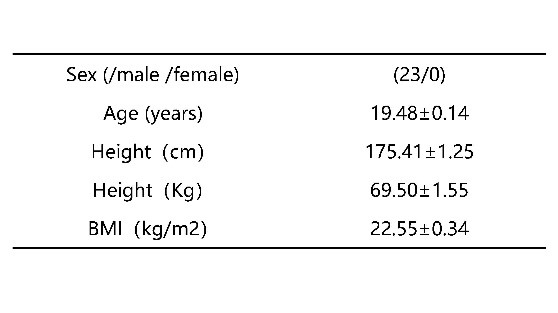
Table 1. General information of study subjects.