2221
Exploring the use of Echo Planar Image Correction (EPIC) for intra operative Diffusion Tensore Imaging. – Initial results1The Intervention Centre, Oslo University Hospital, Oslo, Norway, 2Department of Optometry, Radiography and Lighting Design, University of South-Eastern Norway, Drammen, Norway, 3Department of Neurosurgery, Oslo University Hospital, Oslo, Norway
Synopsis
Intra operative MRI with Diffusion Tensor Imaging allows identification of white mater tracks during surgery allowing for a more aggressive approach by the surgeon while preserving eloquent structures. However DTI is prone to artefacts from B0 inhomogeneity. In this abstract we present our initial experiences on the effect of a commercially available Echo Planar Imaging Correction in the intraoperative setting. While overall image quality is increased, further studies on a larger number of patients are required before the clinical effect can be assessed.
Introduction
Extent of Resection (EOR) is the primary factor determining the survival of patients with glioblastoma, with aggressive resection being strongly correlated with increased post-surgical survival time. [1] However, if the tumor is situated close to eloquent structures such as the white matter tracts (WMT) care must be taken to avoid severe postoperative deficiencies. [1, 2] An accurate evaluation of WMT position relative to gross tumor volume, therefore, allows for increased EOR while preserving neurological functions. Imaging of WTM can be performed using Diffusion Tensor Imaging (DTI) which offers visualization of the tracts. However, due to the EPI readout commonly used in DTI, the images are often influenced by distortion and susceptibility artifacts. In an intraoperative setting, where of-center scanning and suboptimal coils are commonly used, these artifacts become more severe. Recently Philips medical systems have released the technique of “EPIC brain”, which integrates the blip up /blip down approach for EPI-correction directly in the scanner software.At our institution, io-MRI for glioblastoma resection with DTI images is routinely performed. While the EPIC technique is used with much success for routine clinical scanning, we are unaware of any works describing its efficiency during an io-MRI setting. In this abstract, we therefore wish to present our experiences for our first 10 glioblastoma patients using EPIC brain for io-MRI DTI scanning.
Materials and Methods
Patients were informed and consenting. The presented data is a part of a larger project evaluating the biological correlates of MRI sequences. The project is evaluated and approved by the regional ethical board.In the period from March to June 2021 10 patients were scheduled for io-MRI at our institute. Io-MRI was performed following our institution's routines. In short; two multipurpose coils (dStream Flex L, Philips Medical System, Best, The Netherlands) were placed on the patient during anesthesia and the patient was transported to an adjacent 3 Tesla MRI scanner (Philips Medical System, Best, The Netherlands) for imaging. Following imaging, the patients were transported back to the operating room and surgery resumes.
The MRI protocol included 3D-T1w and a DTI sequence (DTI parameters: #slices 18, slice thickness/gap: 4/1mm FOV:230x230 Matrix:160x160 TR/TE: shortest/shortest (approx. 2700/90 ms) #directions: 32). The DTI data were reconstructed both with and without EPIC enabled from the same scan data to allow for direct comparison of IQ. Multi Planar Reconstructions (MPR) were performed on the 3D-T1w sequence using identical geometries as the DTI to serve as ground truth for anatomic structures (Figure 1).
Evaluation of image quality (IQ) was performed by a radiologist (20+ years of experience) assessing; visual noise level, “loss of confidence”, “overall degree of distortion”, “level of artifacts”. All metrics were scored on a 1-5 scale with lower numbers indicating higher IQ. The average IQ for each patient was calculated as the mean of the assessment metrics. In addition, distortion was evaluated using a pseudo method by a radiographer (10+ years experience) where the degree of anatomical fit between the ISO-DTI and the axial T1 MPR was calculated in Nordic ICE (Nordic Neurolabs, Bergen Norway) in a method similar to what is described previously. [3]
The confidence and correlation scores were compared by using a paired samples t-test in Microsoft Excel (Microsoft Corporation, 2010) The difference was considered significant if p-values were <0.05.
Results
Unfortuneatly, one patient was removed from the radiological assessment due to the images being unavailable for the radiologist.Table 1 summarizes the subjective IQ from the radiologist while Table 2 summarizes the average degree of anatomic fit between the DTI images and T1w images.
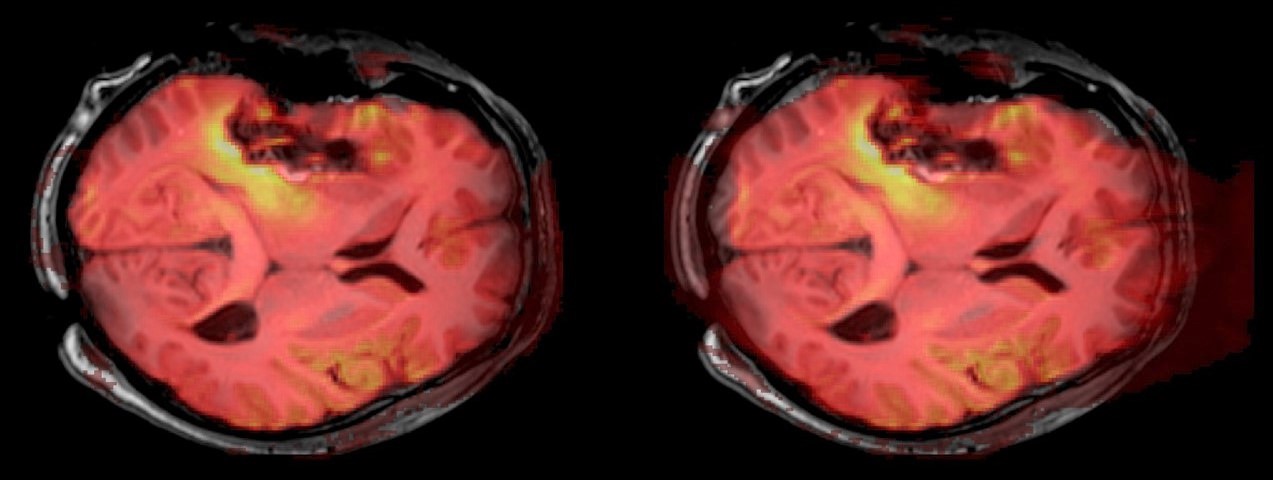
In short; The implementation of EPIC resulted in a significant decrease moise, distortion and a general improvement of IQ. EPIC also increased the anatomic fit between DTI images and T1w-images (Figure 2).
Discussion and Limitations
Average IQ increased with the implementation of the EPIC software, the increase seems to be attributed to the decrease in distortion and noise levels. The increase in anatomic fit seems to validate the radiologist's interpretation of the reduction in distortion as clearly seen in Figures 1 and 2. While the increase in anatomic fit between the corrected and uncorrected image are small, the statistical difference between them is strong. It should be noted, that in Nordic ICE, the degree of correlation is ranged from 1 to 2 where 2 is a perfect fit. Therefore, the small increase in correlation observed in this study might indicate a potential clinical relevance. While there was no significant change in the “loss of confidence” metric, this might be due to a low number of subjects.This study has several limitations, only a small number of patients is included, also we have not assessed the effects of anatomical positioning in the scanner, comparison of DTI vs. other images than T1w or more stringent correlation analysis, such as comparison of structure volumes. In future studies, these metrics should be included and the number of participants should be increased.
Conclusions
Our findings indicate that the use of EPIC has a beneficial effect on io-MRI DTI images and might increase the confidence of WMT positioning. However, the results are based on initial experiences with only a small dataset and should therefore be interpreted with caution.Acknowledgements
No acknowledgement found.References
1. Lacroix, M., et al., A multivariate analysis of 416 patients with glioblastoma multiforme: prognosis, extent of resection, and survival %J Journal of Neurosurgery. 2001. 95(2): p. 190.
2. Rogers, C.M., P.S. Jones, and J.S. Weinberg, Intraoperative MRI for Brain Tumors. Journal of Neuro-Oncology, 2021. 151(3): p. 479-490.
3. Vardal, J., et al., Correction of B0-distortions in echo-planar-imaging-based perfusion-weighted MRI. J Magn Reson Imaging, 2014. 39(3): p. 722-8.
Figures
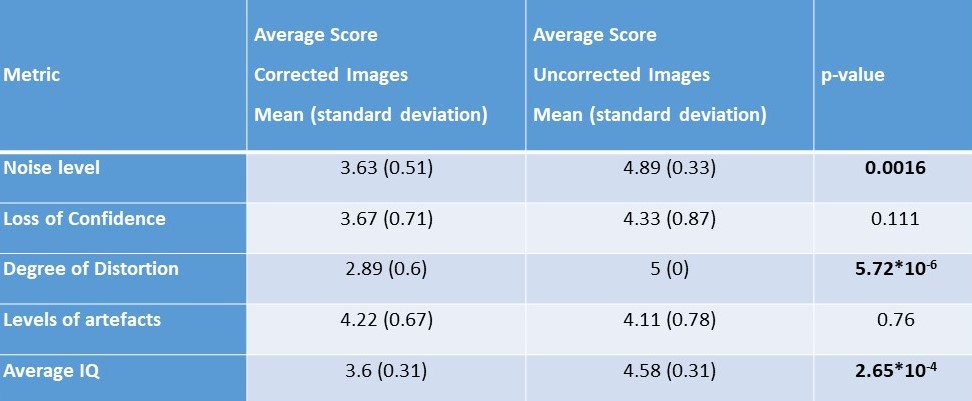
Table 1:
Summary of the results from the subjective reading by the radiologist, significant p-values from paired samples t.test in bold. “Noise level”, “degree of distortions” as well as “average IQ” all improved with the implementation of EPIC. Differences in “loss of confidence” and artifact levels did not achieve significant p-values
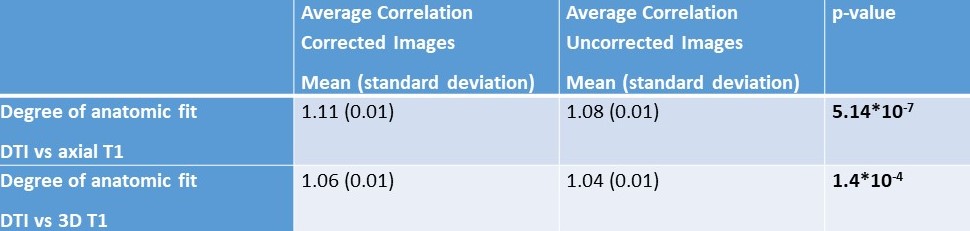
Table 2
Summary of the results from the anatomic fit, significant p-values from paired samples t.test in bold. There was a significant increase in correlation between the DTI images and T1w images, both in the axial MPR’s and the 3D volumetric images.
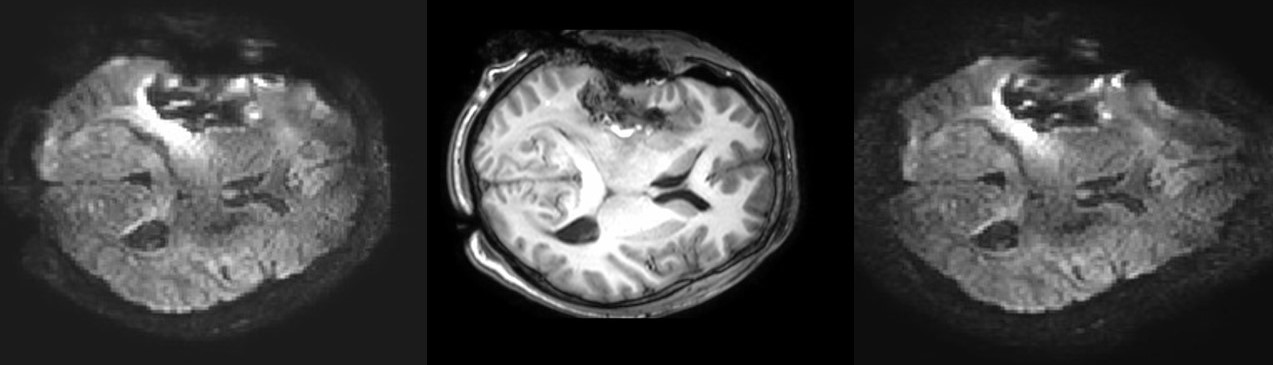
Figure 1.
Representative images showing the DTI sequence with (left) and without (right) Echo Planar Image Correction enabled. T1w-MPR at same slice position (centre) for comparison. The images show a decrease in distortion especially in the anterior part of the brain.