2140
Vendor Independent Visualization Platform for Neuro Device Guidance and Therapeutic Monitoring Based on Stereotactic OR Workstations1Medical Physics, University of Wisconsin-Madison, Madison, WI, United States, 2Radiology, University of California, San Francisco, San Francisco, CA, United States, 3Neurological Surgery, University of Wisconsin-Madison, Madison, WI, United States
Synopsis
The NIH-sponsored international Phase III MISTIE Trial showed that that patients whose residual clot volume was reduced below 15 ml exhibited a statistically higher degree of functional independence. However, CT-image guidance has trouble visualizing clot, brain tissue, and intermediate levels of evacuation. MRI-guidance of ICH evacuations would support far better visualization of clots during attempts at suction or administration of lysing drugs. We present a six panel display whose viewpoints are patterned directly from the Medtronic Stealth workstation. This interface allows for acquisition and display of MR-images in real-time. Viewing planes and image parameters can be changed in real-time.
Introduction
The NIH-sponsored international Phase III MISTIE Trial, which used CT-image guidance to position a catheter at the site of intracerebral hemorrhage (ICH) for periodic clot drainage and infusion of thrombolytic drugs, failed to meet its clinical endpoint for all patients[1]. However, a key finding was that patients whose residual clot volume was reduced below 15 ml exhibited a statistically higher degree of functional independence. Subsequent commercial-sponsored trials using mechanical suction-based devices have also been hindered by the inability to visualize the clot, intermediate levels of evacuation, and nearby brain tissue.MRI-guidance of ICH evacuations would support far better visualization of clots during attempts at suction and/or administration of lysing drugs. Periodic MR assessment of the evacuation process could guide surgeons to reaching the 15 ml residual goal more regularly and quickly. However, surgical adoption of MRI would require an intuitive platform for guiding devices and monitoring therapy that is preferably vendor-independent to simplify training. We present an MRI-guidance platform designed to provide images in real-time from multiple different viewpoints that can be easily adjusted and concurrently displayed. We present a six panel display whose viewpoints are patterned directly from the Medtronic Stealth workstation that neurosurgeons routinely use in the stereotactic OR. Feasibility is demonstrated using in vitro phantom tests beyond our previous computer simulations that used a simpler interface[2].
Methods
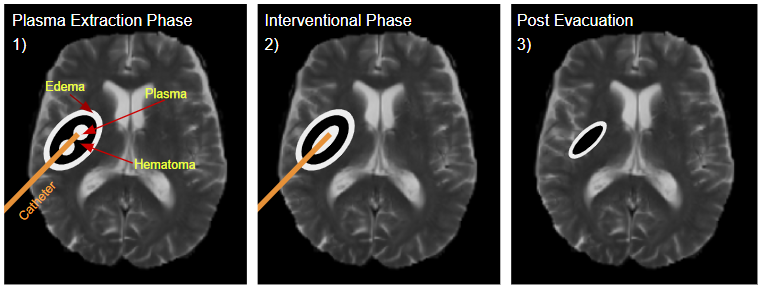
An illustration of high-level tasks in a MRI-guided ICH evacuation procedure is shown in Figure 1. We used the HeartVista RTHawk interventional platform[3], as it permits vendor-independent interventional guidance without requiring in-depth knowledge of each vendor’s software architecture or data pathways. Our interface supports up to 6 concurrent, real-time viewpoints. The user can manually switch between viewpoints or develop an automatic scheduling protocol to update each viewpoint[4]. To mimic the Stealth workstation that is so familiar to neurosurgeons, three viewpoints are co-axial, two views are rotatable about the long axis of the surgical device, and one is perpendicular to the axis of the catheter, termed ‘probe’s eye view’. Two basic imaging experiments were performed:1) Locating and navigating to objects embedded in a phantom during real-time MRI scanning, and 2) Locating and tracking a catheter inserted into a phantom, then monitoring it from 6 different viewpoints.
For all experiments, a 3d-printed half-skull model filled with gelatin representing brain tissue was used as a base as shown in Figure 2. For experiment 1, blueberries were embedded within the gelatin to be located. For experiment 2, chilled pudding encased in plastic was embedded to represent a blood clot with defined boundaries and similar physical properties. A catheter was then introduced. Real-time images were acquired using a 2D GRE where FOV, image orientation, slice thickness, TR, TE and flip angle are all adjustable by the user during scanning.
Results
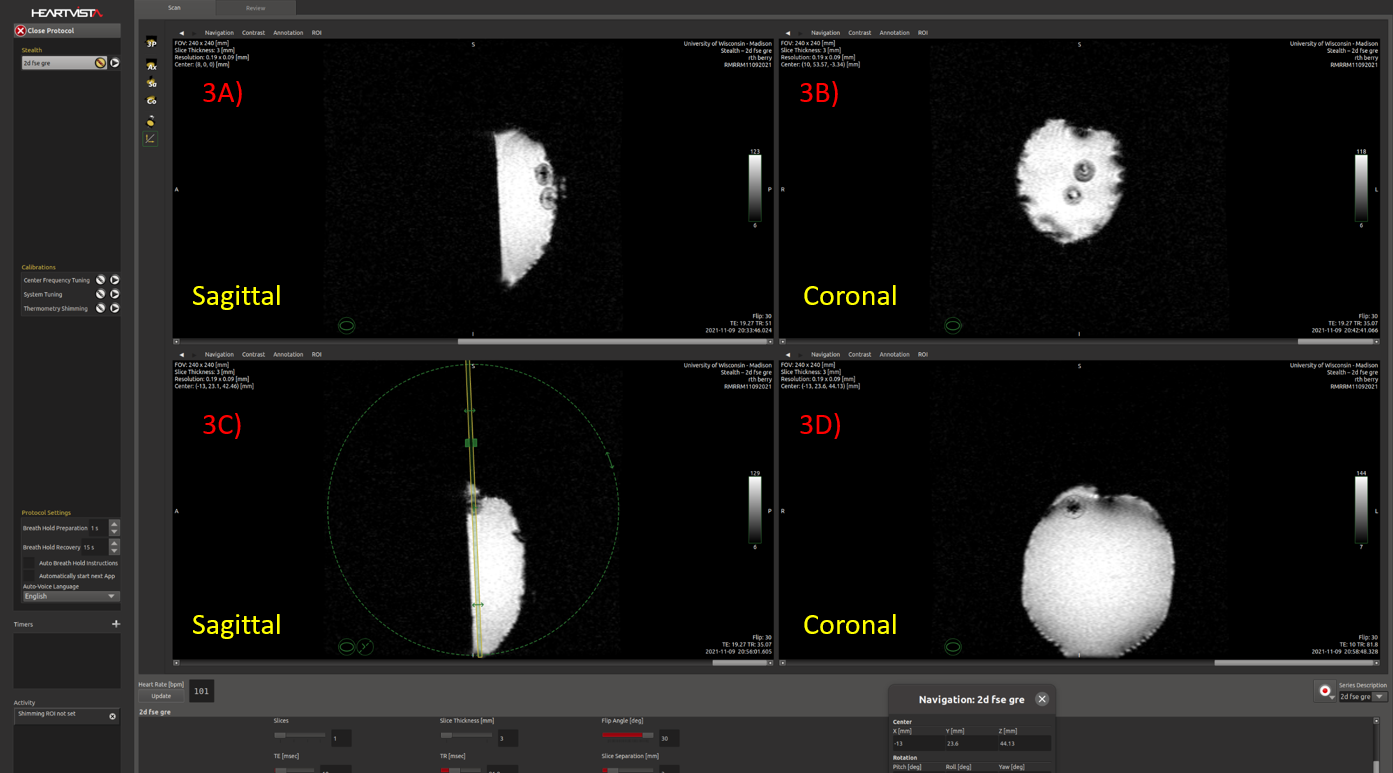
Figure 3 shows the MR-guidance interface where the user has selected four panels to be shown concurrently. Sagittal and axial views are shown, where the top two displays are focused on the berries at the base of the phantom and the bottom displays show the berry situated on the surface. Notice at the bottom of the interface that all parameters including slice prescription can be adjusted in real-time, producing an updated image afterward. Panel 3C shows the use of a through-plane tool. By centering this tool on the object in the presented orientation, Panel 3D automatically populates with a coronal view of the object centered in real-time.Figure 4 shows the full six-panel display. Panel 4A-C are the reference axial, sagittal, and coronal views respectively. Catheter location is either difficult or impossible to see. However, by providing targeting and “skull entry” coordinates, the system can automatically prescribe additional planes co-linear with the catheter such as 4D and 4E. Panel 4F displays the ‘probe’s eye view’ perpendicular to the catheter.
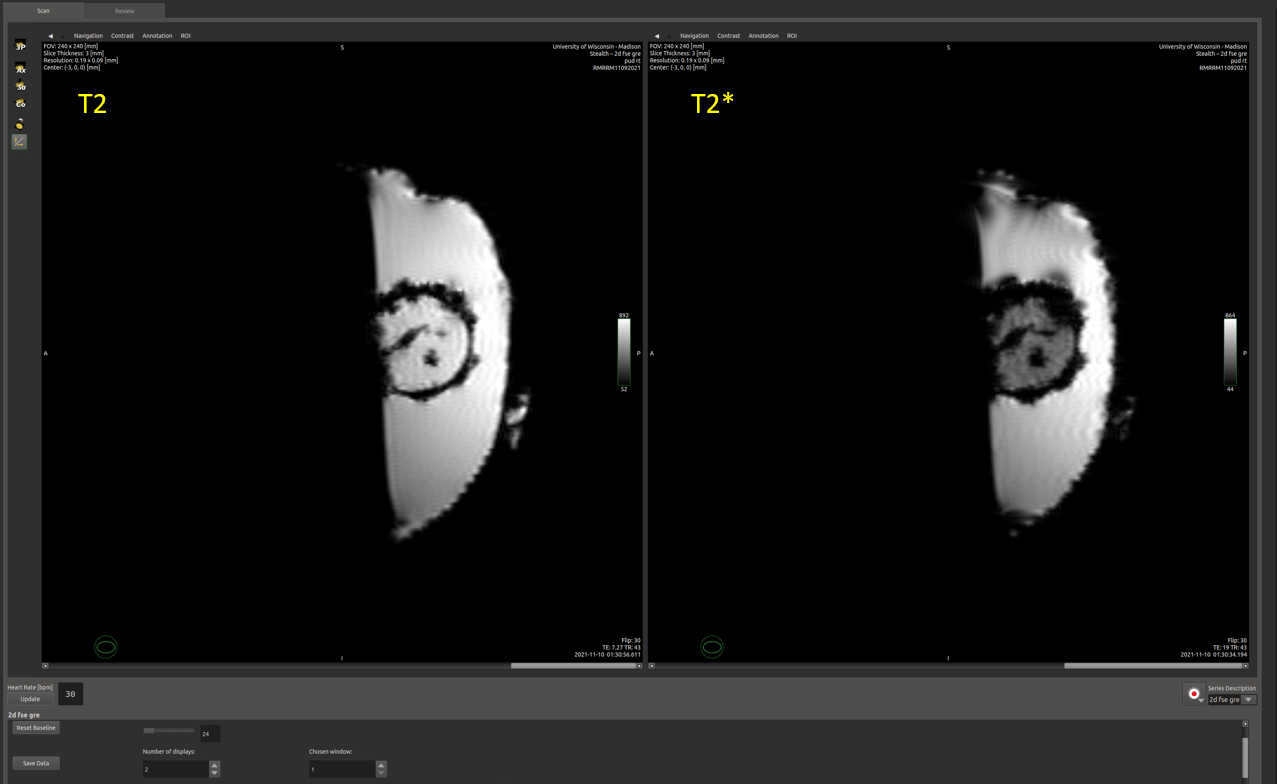
For both figures, each panel shown can be individually adjusted by the user to suit monitoring needs. This includes changing image parameters or image orientation. A different view is easily achievable by using a navigation or through-plane tool. Figure 5 demonstrates two sagittal panels showing catheter placement. Panel 5B was acquired by simply changing the TE and TR values of Figure 5A from 7.2 ms and 43ms to 19ms and 43ms, respectively. The T2* contrast provided by the longer TE highlights the clot.
Discussion
MRI-guidance offers advantages over CT in ICH clot visualization and evacuation. The RTHawk interface gives possibility for MR imaging to be a flexible and reliable real-time guidance tool. Monitoring in the plane of the catheter during administration of lysing drugs, for example, is an intuitive way to monitor the effective progress of these drugs. Our next test model will utilize a full head model with catheters inserted through skull ports. Infusion experiments into real blood clots are planned to determine reliability of tracking drug distribution inside of a clot in real-time.Conclusion
The 6-panel MR-guidance prototype shows potential to be a viable and useful tool to assist and monitor ICH evacuation procedures. Real-time MRI-monitoring in combination with an easy-to-use interface may allow for more extensive and expedient clot evacuation procedures while increasing patient safety.Acknowledgements
No acknowledgement found.References
[1] Hanley DF, Thompson RE, et al. Efficacy and safety of minimally invasive surgery with thrombolysis in intracerebral haemorrhage evacuation (MISTIE III): a randomised, controlled, open-label, blinded endpoint phase 3 trial. Lancet. 2019. Epub 2019/02/12. doi: 10.1016/S0140-6736(19)30195-3. PubMed PMID: 30739747.
[2] Santos JM, Wright GA, Pauly JM. Flexible real-time magnetic resonance imaging framework. Conf Proc IEEE Eng Med Biol Soc. 2004;2:1048-51. PubMed PMID: 17271862.
[3] Moskwa R, Ahmed A, Block W. Prototype Platform for Real-time MR-guided Brain Clot Evacuation. Poster session presented at: ISMRM. 30th Annual Conference. 2021 May 15; Virtual.
[4] Ozhinsky E, Salgaonkar VA, Diederich CJ, Rieke V. MR thermometry-guided ultrasound hyperthermia of user-defined regions using the ExAblate prostate ablation array. J Ther Ultrasound. 2018 Aug 13;6:7. doi: 10.1186/s40349-018-0115-5. PMID: 30123506; PMCID: PMC6088423.
Figures