2137
Initial Observations on the Association of Peri-prostatic Vascular Asymmetry and Extra-prostatic Extension of Prostatic Tumors1Division of Radiology, IEO, European Institute of Oncology IRCCS, Milano, Italy, 2University of Milan, Milano, Italy, 3Uropathology and Intraoperative Diagnostics, IEO, European Institute of Oncology IRCCS, Milano, Italy, 4Department of Oncology and Hemato-oncology, University of Milan, Milano, Italy, 5Division of Urology, IEO, European Institute of Oncology IRCCS, Milano, Italy, 6Division of Radiation Oncology, IEO, European Institute of Oncology IRCCS, Milano, Italy, 7Precision Imaging and Research Unit, IEO, European Institute of Oncology IRCCS, Milano, Italy
Synopsis
We hypothesized that the presence of asymmetry in the arterial supply of the prostate may provide a correlate of extra-prostatic tumor extension in patients with prostate cancer. In this preliminary study of 40 patients (20 with and 20 without extra-prostatic disease), a radiologist blind to the status of the patients, made a binary choice as to the presence or absence of peri-prostatic vascular asymmetry. Taking the pathological grading as the reference standard, the sensitivity, specificity, positive and negative predictive values were all 0.9. The negative likelihood ratio (LR-) was 0.11, and the positive likelihood ratio (LR+) was 9.0.
Introduction
Multiparametric magnetic resonance imaging of the prostate has taken a central role in the diagnostic assessment of prostate cancer, with the Prostate Imaging, Reporting and Data System (PI-RADS) (v2.1) currently providing a framework for assessment. In the assessment of extracapsular disease.1 Nonetheless, while a low PI-RADS assessment category is effective in excluding extra-prostatic extension,2 there remains room for improvement in deciding whether extra-prostatic extension is present when disease is more significant.3Several studies have shown an increase in MRI-visible blood vessels in the breasts containing tumors compared to the contralateral breast.4-6 We hypothesized that a similar asymmetry in the periprostatic vasculature may be indicative of extra-prostatic extension of prostate cancers.
Our aim was to evaluate whether asymmetry in the depiction of vessels seen via dynamic contrast enhanced MRI was related to extra-prostatic disease at final histology after prostatectomy.
Methods
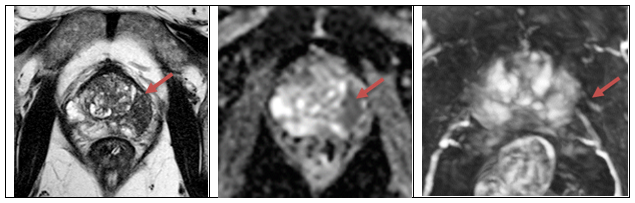
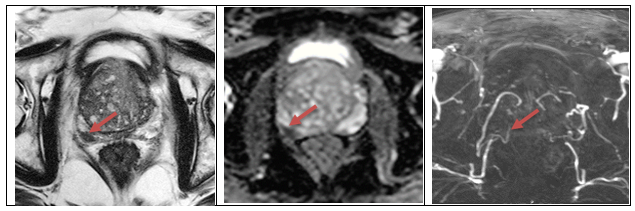
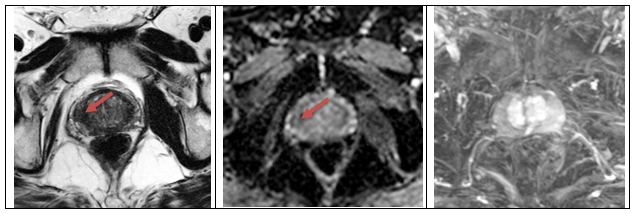
In this ethical committee-approved retrospective study, following an initial review of 16 cases to identify the approximate incidence of vascular asymmetry in patients with and without extra-prostatic disease, a separate cohort was formed of 40 consecutive patients who underwent PI-RADS compliant 3T MRI (Skyra, Siemens Healthineers, Erlangen Germany) of the prostate between January and November 2019, and subsequent prostatectomy, both within our institution With the axial T2- and diffusion-weighted images and ADC maps for anatomical and radiological reference, but blinded to prior radiological and pathological reports, a radiologist evaluated whether there or not was an increased number or caliber of the feeding arteries ipsilateral to the index lesion (referred to as vascular asymmetry) on maximum intensity projection (MIP) images, reconstructed from the dynamic contrast enhanced (DCE) compared with the contralateral side.Results
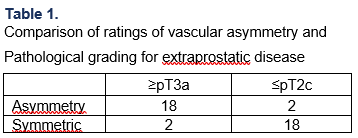
The 40 patients formed two distinct populations: 20 cases with tumor limited to the prostate (2 cases pT2b, 18 cases pT2c) and 20 cases with extra-prostatic tumor at definitive histology (4 cases pT3b, 16 cases pT3a). Illustrative examples of cases where the peri-prostatic vessel asymmetry status was considered a true-positive, false positive and false negative in light of pathology pT status are shown in Figures 1 -3 respectively.The presence of peri-prostatic vascular asymmetry concorded with the pathological assessment of extracapsular disease in 18 of 20 patients (pT3a or pT3b), while its absence corresponded to gland-limited disease (pT2a or pT2b) in 18 of 20 patients (Table 1). There was discordance between the vascular asymmetry and pathology assessment in 2 cases of extra-prostatic disease and two cases of gland-limited disease. Correspondingly, sensitivity, specificity, positive predictive value (PPV), and negative predictive value (NPV) were all 0.9. The negative likelihood ratio (LR-) was 0.11, and the positive likelihood ratio (LR+) was 9.
The χ2-test showed a significant difference in the frequency of vascular asymmetry between the two groups (χ2=24.96, p<0.0001).
Discussion
A recent review found that the majority of the tools for prediction of extra-prostatic extension of prostate cancer are unlikely to be appropriate for patients' counselling or for surgical strategy preplanning 3. The sensitivity, specificity, PPV, NPV. PR- and LR+ for the prediction of extracapsular extension of prostate cancer based on vascular asymmetry in our cohort were 0.9, 0.9, 0.9, 0.9, 0.11, and 9.0. This high level of diagnostic performance warrants further investigation as a possible means of addressing one of the weaknesses of current pre-surgical assessment in prostate cancer.The size of the cohort in this single-center study, and the reading by a single radiologist are limitations to the possible generalizability of the findings. The reading of the MIP images was performed in combination with the T2, DWI and ADC images as we expect would be the case in clinical practice. We note that without referring to the diagnostic images for localization of the tumor, the radiologist felt the ability to distinguish vascular asymmetry from the MIPs alone would be greatly reduced, and that the evaluation of vascular asymmetry is likely to be highly subjective. We have initiated work on an automated assessment of perivascular enhancement to reduce this variability. We expect that in studies of prospective populations, characterized by lower prevalence of extra-prostatic disease, the diagnostic performance of these semeiotic MR features may improve.
Conclusion
This preliminary study suggests that alterations to the peri-prostatic vasculature are present in prostate cancer patients, and may be more evident in those with extra-prostatic disease. The observed ability of the absence or presence of peri-prostatic vascular asymmetry in ruling out or ruling-in the presence of extra-prostatic disease exceeds recent reports on the performance of the widely used PI-RADS system. Further investigation of the possible use of vascular asymmetry in evaluating prostate cancer for extra-prostatic extension is therefore warranted.Acknowledgements
No acknowledgement found.References
1. Turkbey B, Rosenkrantz AB, Haider MA, et al. Prostate Imaging Reporting and Data System Version 2.1: 2019 Update of Prostate Imaging Reporting and Data System Version 2, Eur Urol. 2019;76(3):340–351.
2. Alessi S, Pricolo P, Summers P, et al. Low PI-RADS assessment category excludes extraprostatic extension (≥pT3a) of prostate cancer: a histology-validated study including 301 operated patients. Eur Radiol. 2019;29(10):5478-5487.
3. Rocco B, Sighinolfi MC, Sandri M, et al. Is Extraprostatic Extension of Cancer Predictable? A Review of Predictive Tools and an External Validation Based on a Large and a Single Center Cohort of Prostate Cancer Patients. Urology. 2019;129:8-20.
4. .Verardi N, Leo G, Carbonaro LA, Fedeli M, Sardanelli F. RM mammaria con mezzo di contrasto: Associazione tra incremento asimmetrico della vascolarizzazione e tumore ipsilaterale in una serie consecutiva di 197 pazienti, Radiol Medica. 2013;118(2):239–250.
5. Schmitz AC, Peters NHGM, Veldhuis WB, et al. Contrast-enhanced 3.0-T breast MRI for characterization of breast lesions: Increased specificity by using vascular maps, Eur Rad. 2008;18(2):355–364.
6. Mahfouz AE, Sherif H, Saad A, et al. (2001) Gadolinium-enhanced MR angiography of the breast: Is breast cancer associated with ipsilateral higher vascularity?, Eur Radiol. 2001;11(6):965–969.
Figures