2110
Cerebellum structural and functional connectivity alteration in relation to freezing of gait in Multiple system atrophy1Renmin Hospital of Wuhan University, Wuhan, China, 2GE Healthcare, Beijing, China
Synopsis
Cerebellum is responsible for posture and gait control. 67% of patients with multiple system atrophy experienced FOG. Patients with the damaged cerebellar locomotor region had gait-freezing-like symptoms, suggesting that the cerebellum may be involved in the occurrence and development of FOG symptoms. This study suggested that the cerebellum volume atrophy may be involved in FOG development in MSA patients and subsequently induce functional abnormality in the cerebellum-cerebral circuit. This study provided neuroimaging evidence for clinical understanding of cerebellum role in MSA patients with FOG injury.
Introduction
Multiple system atrophy (MSA) is a sporadic, adult-onset neurodegenerative disease characterized by autonomic failure, parkinsonism, and symptoms of cerebellar ataxia [1]. Freezing of gait(FOG)was defined as“Brief, episodic absence or marked reduction of forward progression of the feet despite the intention to walk [2]. The previous epidemiological study has shown that 67% of patients with multiple system atrophy experienced FOG. Severe freezing of gait may cause falling and disability, thereby accelerating disease progression and increasing burden on caregivers. At present, the mechanism of MSA with FOG symptoms is unclear which hinders clinicians from understanding the full picture of the disease. Neuroimaging studies found that besides pedunculopontine nucleus the cerebellum is also widely involved in fog regulation in patients with Parkinson's disease [3]. A recent study further found that patients with the damaged cerebellar locomotor region had gait-freezing-like symptoms [4], suggesting that the cerebellum may be involved in the occurrence and development of FOG symptoms. Due to the key role of the cerebellum impairment in MSA, the current study was to explore whether atrophy of cerebellar gray matter volume and cerebellum-cerebral circuit related to FOG in multiple system atrophy patients.Materials and Methods
59 MSA patients with FOG and 30 MSA patients without FOG diagnosed by Parkinson's disease clinic doctors and confirmed by follow-up study were included in this study. All patients underwent the resting state function magnetic resonance BOLD sequence and T1 BRAVO structural image 3.0T MRI scanner (Discovery MR750W, GE Healthcare). The changes of cerebellum subregion volume and cerebellum atrophy secondary cerebellum-cerebral circuit were analyzed by SPM12 software embed in MATLAB. The relationship between these changes and the severity of FOG score was further analyzed.Results
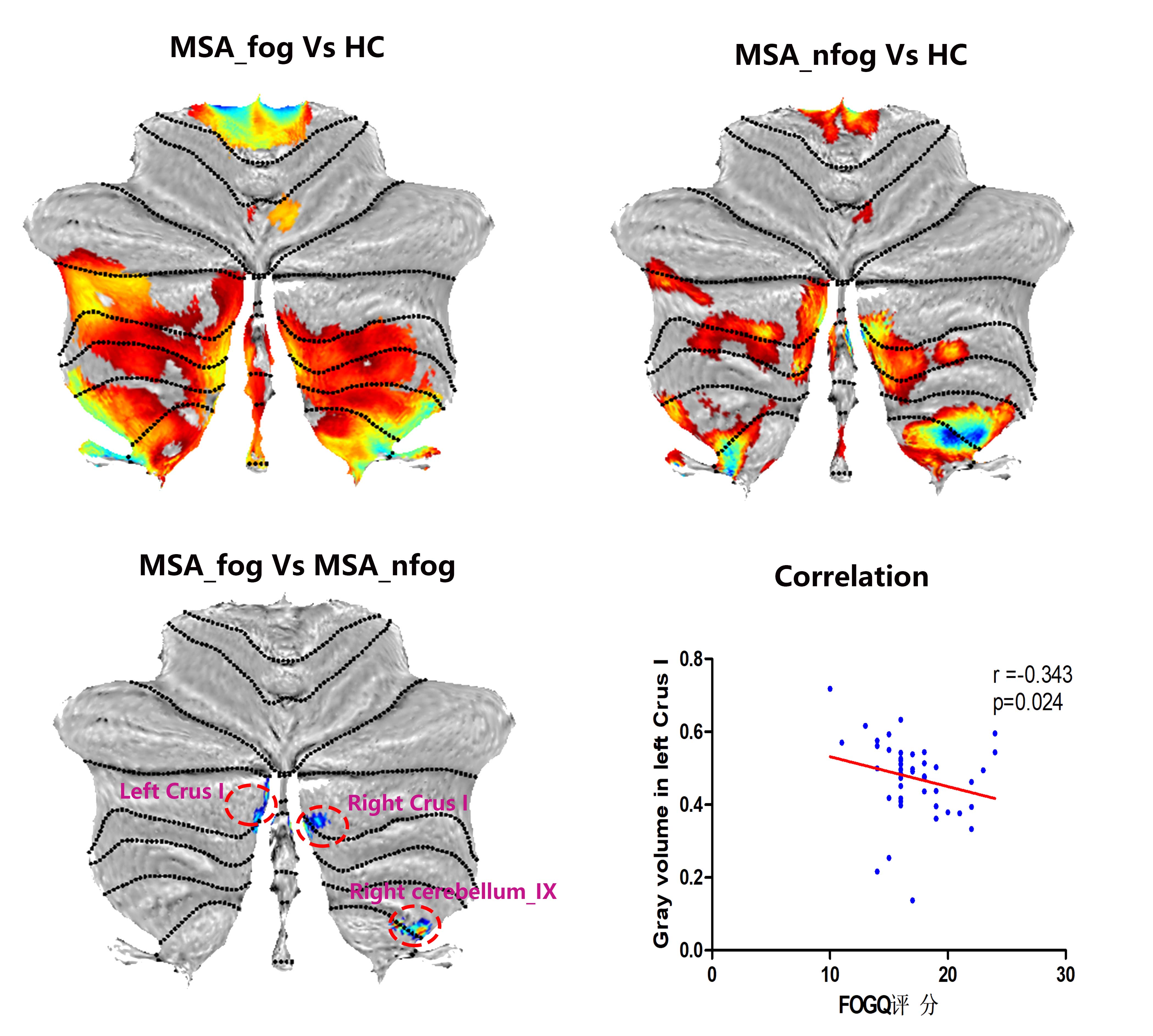
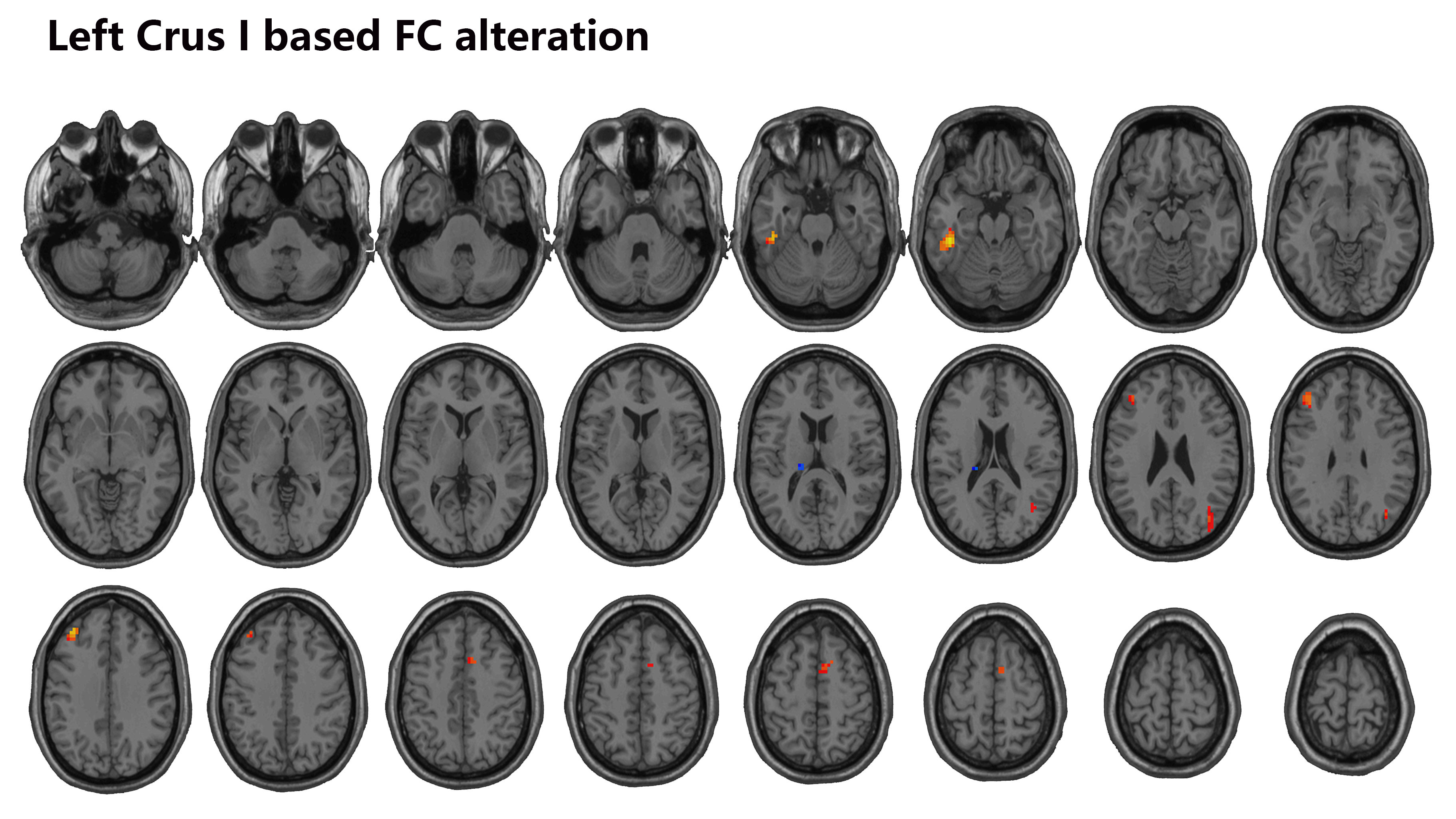
The volume shrinkage in the left cerebellum_Crus I was the main manifestation of MSA patients with FOG injury, which was negatively correlated with the severity of gait freezing (Figure 1). A secondary FC analysis based on the left cerebellum_Crus I as a seed revealed a decreased functional connectivity between the left cerebellum_Crus I and left inferior temporal gyrus, left thalamus, right middle occipital gyrus, left middle frontal gyrus and right supple motor areas. The gray volume decreased in left cerebellum_crus I and “cerebellum-cerebral” circuit functional connectivity dysfunction from left cerebellum_Crus I to left inferior temporal gyrus, left thalamus, right middle occipital gyrus, left middle frontal gyrus and right supplementary motor area.Discussion
We found MSA patients with or without fog showed significant different cerebellar gray matter volume after controlling the interference of motor and non-motor covariates. This suggested that cerebellar atrophy may be involved in the regulation of fog symptoms in MSA patients, which is distinct from idiopathic PD patients with fog injury, inconsistent with many studies holding the view that the cerebellar function was abnormal rather than cerebellar gray matter structure alteration involved in FOG regulation. In present study, MSA patients with FOG symptoms showed more widely cerebellum subregion injury, including bilateral Crus I and right cerebellum_IX, than those without FOG. Left cerebellum_Crus I was the only cerebellum region related to FOG severity in MSA patients. Furthermore, a second seed-based functional connectivity method revealed the frontal lobe, supplementary motor and thalamus in a “cerebellum-cerebral” circuit were impaired. In the walking conditions, the cerebellar crus I plays a role in executive control by receiving information from the middle frontal fields. The relationship between the FOG severity and decreased the cerebellum Crus I volume as well as weaker cerebellum-cerebral circuit in the present study may explain that disturbances of executive control in loading task can exacerbate the gait freezing.Conclusions
This study suggested that the cerebellum volume atrophy may be involved in FOG development in MSA patients and subsequently induce functional abnormality in the cerebellum-cerebral circuit. This study provided neuroimaging evidence for clinical understanding of cerebellum role in MSA patients with FOG injury.Acknowledgements
No acknowledgement found.References
1. Fanciulli A, Wenning GK: Multiple-system atrophy. N Engl J Med 2015, 372(3):249-263.
2. Lord SR, Bindels H, Ketheeswaran M, Brodie MA, Lawrence AD, Close JCT, Whone AL, Ben-Shlomo Y, Henderson EJ: Freezing of Gait in People with Parkinson's Disease: Nature, Occurrence, and Risk Factors. J Parkinsons Dis 2020, 10(2):631-640.
3. Jung JH, Kim BH, Chung SJ, Yoo HS, Lee YH, Baik K, Ye BS, Sohn YH, Lee JM, Lee PH: Motor Cerebellar Connectivity and Future Development of Freezing of Gait in De Novo Parkinson's Disease. Mov Disord 2020, 35(12):2240-2249.
4. Fasano A, Laganiere SE, Lam S, Fox MD: Lesions causing freezing of gait localize to a cerebellar functional network. Ann Neurol 2017, 81(1):129-141.
Figures