2098
Comparison of ultra-high field MRI of ancient remains at 9.4T and 3T1Dept.of Radiology, Medical Physics, Medical Center University of Freiburg, Faculty of Medicine, University of Freiburg, Freiburg, Germany, 2Department of Neurosurgery, Section for Neuroelectronic Systems, University Medical Center Freiburg, Freiburg, Germany, 3Institute of Evolutionary Medicine, Faculty of Medicine, University of Zurich, Zurich, Switzerland
Synopsis
Ancient mummified samples have ultra-short T2* which decreases with increasing field strength. Here, image quality and T2* relaxation times are compared for different tissues of a mummified hand between a clinical 3T and a preclinical 9.4T system using a 3D UTE sequence. Although T2* is shorter at 9.4T, image quality was superior to 3T, justifying the benefits of ultra-high fields (UHF).
Introduction
In paleoradiology, X-ray based non-invasive imaging modalities such as CT are predominantly used to image the rare and fragile ancient remains. MRI of specimen such as mummified samples is difficult due to the low proton density and the extremely short T2* of the mummified tissue. Thus, the attainable SNR and the spatial resolution are limited with MRI, even though very long measurement times can be realized. To overcome the rapid T2*decay, pulse sequences such as ultra-short echo time (UTE) or pointwise encoding time reduction with radial acquisition (PETRA) are used. These sequences provide improved contrast of mummified tissue, and they can be applied to quantify the relaxation times1-3. However, they depend heavily on suitable hardware with dedicated RF coils4 and fast Tx/Rx switching as well as high performance gradients to maximize SNR. Recently, MRI of ancient remains was shown with custom-made gradient inserts5 at 3T. In this work, we investigate the benefits of ultra-high field (UHF) at 9.4T against clinical fields (3T).Materials and Methods
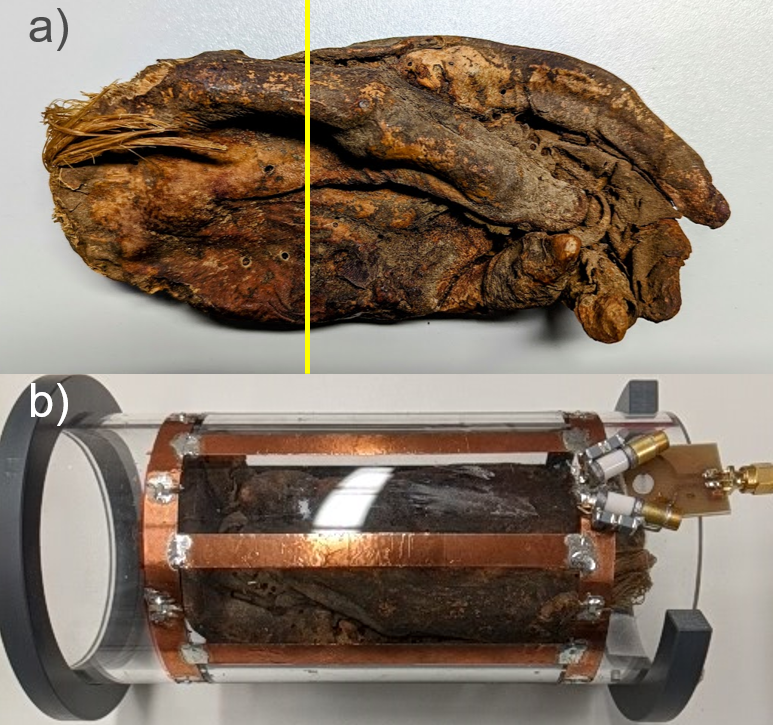
An embalmed ancient Egyptian mummified left hand (approx. 1500–1100 BC) was used for MRI measurements (former collection of musée d’Orbe, Switzerland; Fig.1). The hand was imaged with a preclinical MRI system at 9.4T (Bruker BioSpec 94/20 USR, Ettlingen, Germany) with a bore size of 20 cm, that offers a gradient system with Gmax=724 mT/m and a slew rate of 4570 T/(m s). A custom-built linear Tx/Rx high pass birdcage coil (diameter: 9 cm, 8 legs, length: 13.5 cm, leg length: 11.5cm, leg width: 9mm, Q-factor:144, f0=400 MHz) was used. For comparison, MRI data of the same sample were acquired at a clinical 3T system (PrismaFit, Siemens, Erlangen) with Gmax=80 mT/m and a slew rate of 200 T/(m s) and a dedicated Tx/Rx low pass birdcage coil in quadrature mode (f0=123.2 MHz, Q factor: 150). At 9.4T, a 3D UTE sequence was used for imaging with following parameters: TE = 40, 80, 160, 320, 640 µs, TR=5 ms, FA=4°, FOV=80mm, 10 averages, reconstructed to a matrix size of 1603, bandwidth of 625 Hz/Pixel, 80000 spokes, an isotropic resolution of 0.5mm and TA of 68 min. A T2* map was calculated from the 5 different TEs by a mono-exponential fit. At 3T, a 3D UTE sequence was applied with the following parameters: TE=70, 120, 250, 400, 800µs, TR=5ms, FoV=192mm, 10 averages, matrix size of 384³, BW=625 Hz/Pixel, FA=16°, 80000 radial spokes, isotropic resolution of 0.5mm and TA=68 min.Results
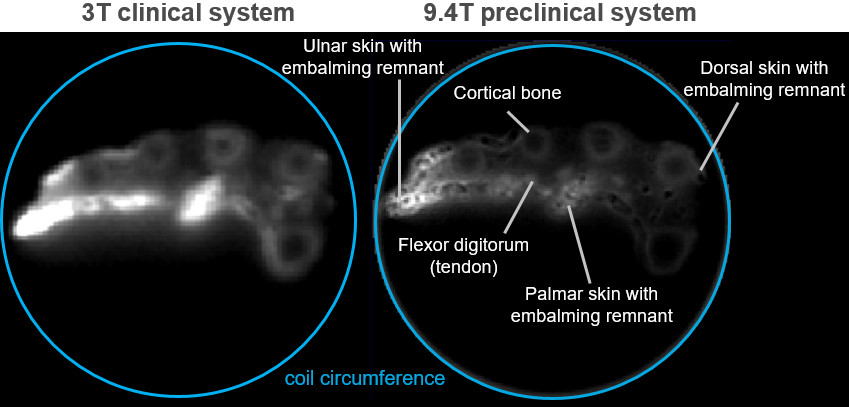
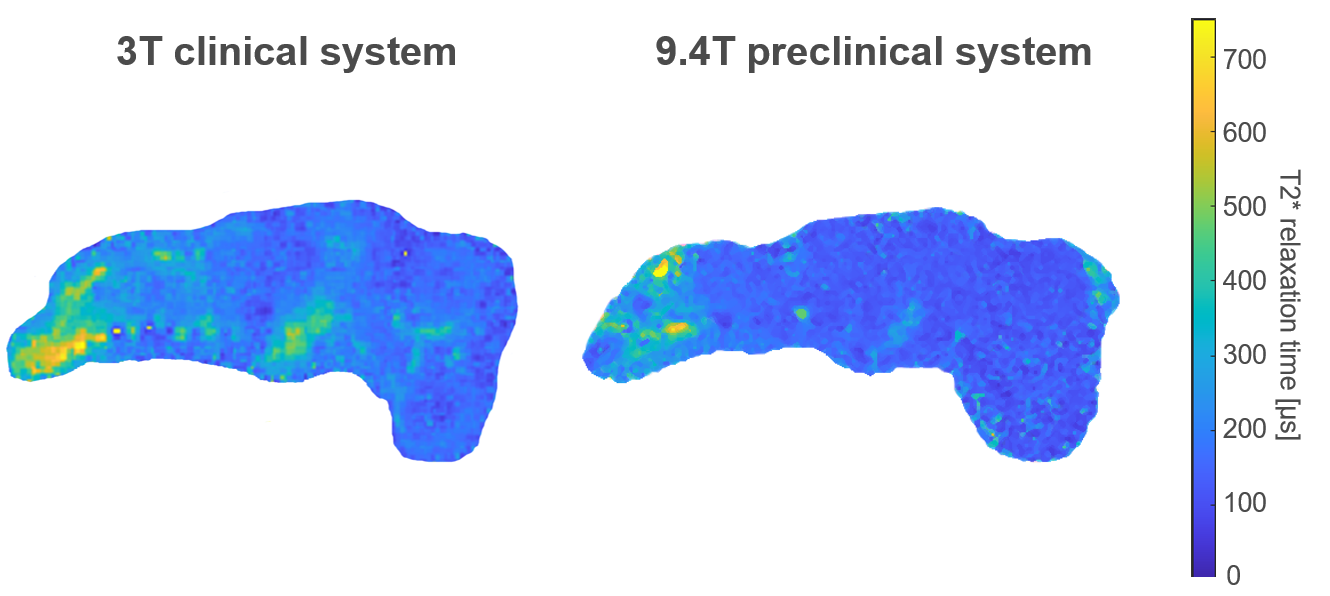
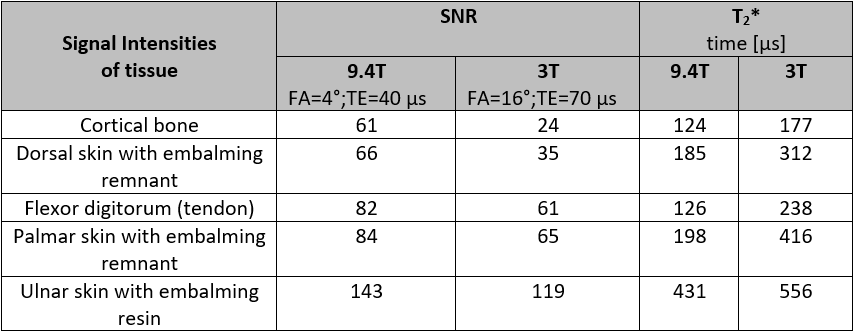
A transverse slice at the base of the hand from the data sets at 3T (TE=70µs) and 9.4T (TE=40µs) is marked and shown in Fig. 2. Anatomical details such as the cortical bone, tendons, and skin with embalming remnants are identifiable at both field strengths. The 9.4T system has a higher performance gradient system, thus the images suffer less from T2* induced blurring. Cortical bone (SNR9.4T=61, SNR3T=24) and dorsal skin (SNR9.4T=66, SNR3T=35) yield the highest SNR gain. For most tissues, the SNR is superior for the 9.4T system, despite reduced T2* relaxation time. Ulnar skin with embalming remnant gives the highest SNR9.4T=143 compared to 119 at 3T. The T2* map (Fig. 3) also shows the highest relaxation time for skin with embalming resin (T2*=431µs at 9.4T, T2*=556µs at 3T). The range of T2* relaxation times is reduced to below 200µs for all tissues at 9.4T besides ulnar skin, whereas at 3T the T2* relaxation times have a much broader range (177µs to 556µs) (Table 1).Discussion
Imaging at a preclinical UHF MRI system provides highly improved image quality in terms of SNR and image sharpness for short T2* samples. Increased SNR unveils more anatomical details and alteration of T2* relaxation time might also provide additional contrast insight. This is possible due to improved hardware specifications which allow a much shorter TE (40µs at 9.4T system compared to 70µs at clinical 3T) yielding an SNR improvement of up to 20%. Additionally, preclinical systems employ much stronger gradients than clinical systems. This enables rapid encoding, shortening the readout time after RF excitation that increases image sharpness of samples with very short T2*. Higher B0 field strength provides significant sensitivity gain for improved SNR. At clinical systems, much more sequence optimization steps are required to obtain high image quality such as ideal Ernst angle (using FA=4° at 3T - identical to 9.4T - the measured signal was extremely low). However, there are several downsides such as the simultaneous decrease of T2* relaxation times down to 50% compared to 3T, that reduces SNR. Another aspect is the smaller bore size (20cm diameter) and and narrow range of gradient linearity (approximately 5-6cm in z-direction) in comparison to clinical devices. This requires precise placement in the iso-center of the scanner to circumvent any off-center effects due to the radial sequence and to obtain full FoV coverage. Thus, these space limitations constrain the measurements to smaller specimen.Conclusion
In summary, MRI of ancient remains can be performed with improved image quality at ultra-high field systems despite the shorter T2* times and the sample size limitations. These MRI acquisitions with spatial resolution up to 0.5mm would allow a detailed analysis of anatomical structures providing additional insight and supplement other imaging modalities such as CT.Acknowledgements
Grant support from the Deutsche Forschungsgemeinschaft (DFG) under grant numbers BO 3025/8-1 and UL 1187/6-1 is gratefully acknowledged.References
1. Münnemann K, et al. Magn Reson Imaging 2007; 25(9): 1341-5.
2. Öhrström LM, et al. "Scenes from the past: MR imaging versus CT of ancient Peruvian and Egyptian mummified tissues." Radiographics 33.1 (2013): 291-296.
3. Özen AC, et al. "Comparison of ultrashort echo time sequences for MRI of an ancient mummified human hand." Magnetic resonance in medicine 75.2 (2016): 701-708.
4. Tesfai AS, et al. "Multi-parameter Analytical Method for B1 and SNR Analysis (MAMBA): An open source RF coil design tool." Journal of Magnetic Resonance 319 (2020): 106825.
5. Baadsvik, EL, et al. "High‐resolution MRI of mummified tissues using advanced short‐T2 methodology and hardware." Magnetic Resonance in Medicine 85.3 (2021): 1481-1492.
Figures