2040
MRI Tagging of Colonic Contents in Healthy Subjects: Reliability of the Measurement with Time1Translational Medical Sciences and National Institute for Health Research (NIHR) Nottingham Biomedical Research Centre, Nottingham University Hospitals NHS Trust and University of Nottingham, Nottingham, United Kingdom, 2Department of Diagnostic Radiology, College of Applied Medical Sciences, University of Hail, Hail, Saudi Arabia, 3NIHR Nottingham Biomedical Research Centre (BRC), Nottingham University Hospitals NHS Trust and University of Nottingham, Nottingham, United Kingdom, 4Sir Peter Mansfield Imaging Centre, School of Physics and Astronomy, University of Nottingham, Nottingham, United Kingdom
Synopsis
We aimed to investigate the temporal variation of the MR colonic tagging technique to measure mixing of colonic contents following a water based laxative drink by acquiring multiple scans on healthy participants. The study results indicate that time did not influence the measurement of colonic content mixing, however the scans were variable over the 10 minute acquisition window which suggests multiple scans are needed to accurately assess this parameter. Multiple measurements of this non-invasive technique can be used in future studies that aim to look at bowel motility and treatment response of IBD patients, using the same water-based laxative.
INTRODUCTION
Colonoscopy is the gold standard for objective assessment of colonic disease activity in Crohn’s disease (CD) and ulcerative colitis (UC). However, only 75% of patients are willing to have this invasive assessment procedure repeatedly, while only 60% of them consider colonoscopy as an acceptable experience1. Recently investigators have used MRI to examine the effects of CD inflammation on bowel motility, finding a reduction in small bowel motility that was linked to the inflammation 2. Non-invasive colonic imaging using MRI may have a role in quantifying different aspects of colonic disease activity and bowel motility. In this study, we aimed to investigate the temporal variation and hence reliability of the colonic tagging technique (proposed by Pritchard et al.3) used to measure dynamic mixing of colonic contents by acquiring multiple measurements over time on healthy participants. This will inform future protocols to accurately assess colonic content mixing in prospective cohort studies of inflammatory bowel disease patients.METHODS
Healthy participants (without any history of gastrointestinal disease or use of medication known to affect gastrointestinal transit) were scanned using a 3T Philips Achieva MRI scanner (Philips, Best, The Netherlands). Participants arrived at the test centre fasted and were given 1000 mL of oral bowel preparation (2.5% mannitol with 0.2 % locust bean gum), to ingest slowly over 40 minutes. The scanning session was performed two hours after participants started consuming the oral contrast (t=120 minutes). A schematic of study pathway is illustrated in figure 1. The MRI tagging scans were positioned to cover the central ascending colon (AC) with 10 independent measurements over time, with scans acquired at 1 minute intervals. Each tagging scan to assess the motion of the colonic contents was a 20 seconds cine breath-hold balanced turbo field echo (bTFE) sequence, with a single 15mm thick sagittal oblique slice placed through the AC, dark horizontal strips (tag lines) were 12 mm apart (FOV= 330 x 259 mm2; resolution = 0.98 x 0.98 mm2; FA = 45°). The mean and the standard deviation (std dev) maps of AC (figure 2) were generated pixel-by-pixel using custom-written software3 in MATLAB. The colonic regions of interest (ROIs) were defined using MIPAV software4 using the mean map as the reference image, and the resulting coefficient of variation (%CoV) defined as: ROI signal stdev map*100/ROI signal mean map was calculated3. Mixing of contents results in movement and smearing of the tag lines and result in larger standard deviation values increasing the CoV. For each tagging scan, a different (individual) ROI around the colon region was drawn and %CoV measured. The mean and std dev of all repeated measures for each subject were calculated along with mean and std dev for the first 5 and last 5 time points separately. To determine whether there was any increase in the variability of the measurement with increased %CoV (increased mixing) the Pearson Correlation coefficient was calculated. To investigate whether there was any trend in the data acquisition with time, a one-way repeated measure ANOVA analysis was conducted using SPSS.RESULTS
Nine participants were recruited: four female, five male, mean age 29 (std dev 10) years old. The change over time between the multiple measurements of the mixing of the colonic contents due to variations in colonic content mixing is shown in figure 3. Mean and std dev of the calculated %COV for each subject are shown in table 1. Data is calculated for all 10 repeated scans, then first five, and last five scans, respectively. These data don’t show any obvious consistent time variation between the multiple measures. The correlation between the mean and std dev of the ten scans is shown in figure 4. The direction of the relationship is positive, meaning that these variables tend to increase together (Pearson r=.510, P = 0.161 for a two-tailed test). There was no significant difference found between the multiple measures with time (P = 0.61, one-way repeated measures ANOVA test).DISCUSSION & CONCLUSION
The results of this small scale study indicate that the time of acquisition did not influence the measurement of colonic content mixing, however the values measured showed some variability over the 10 minute acquisition window which suggests multiple measurements are needed to accurately assess this parameter. 8 out of 9 subjects had their mean first 5 and last 5 scans within one std dev of all the scans mean which indicates that 5 scans could be sufficiently accurate. Within-subject measurements of all the ten colonic tagging scans show a slight trend for increased std dev with increasing mean %CoV which indicates that the variation increases slightly with increased colonic content mixing. Multiple measurements of this non-invasive technique can be used to in future studies that aim to look at bowel motility and treatment response of IBD patients, using the same water-based laxative.Acknowledgements
No acknowledgement found.References
- Miles A, Bhatnagar G, Halligan S, et al. Magnetic resonance enterography, small bowel ultrasound and colonoscopy to diagnose and stage Crohn’s disease: patient acceptability and perceived burden. European Radiology. 2019;29(3):1083-1093.
- Plumb AA, Menys A, Russo E, et al. Magnetic resonance imaging-quantified small bowel motility is a sensitive marker of response to medical therapy in Crohn's disease. Aliment Pharmacol Ther. 2015;42(3):343-355.
- Pritchard SE, Paul J, Major G, et al. Assessment of motion of colonic contents in the human colon using MRI tagging. Neurogastroent Motil. 2017;29(9).
- McAuliffe M, Lalonde F, McGarry DP, Gandler W, Csaky K, Trus B. Medical Image Processing, Analysis & Visualization in Clinical Research. Vol 142001.
Figures

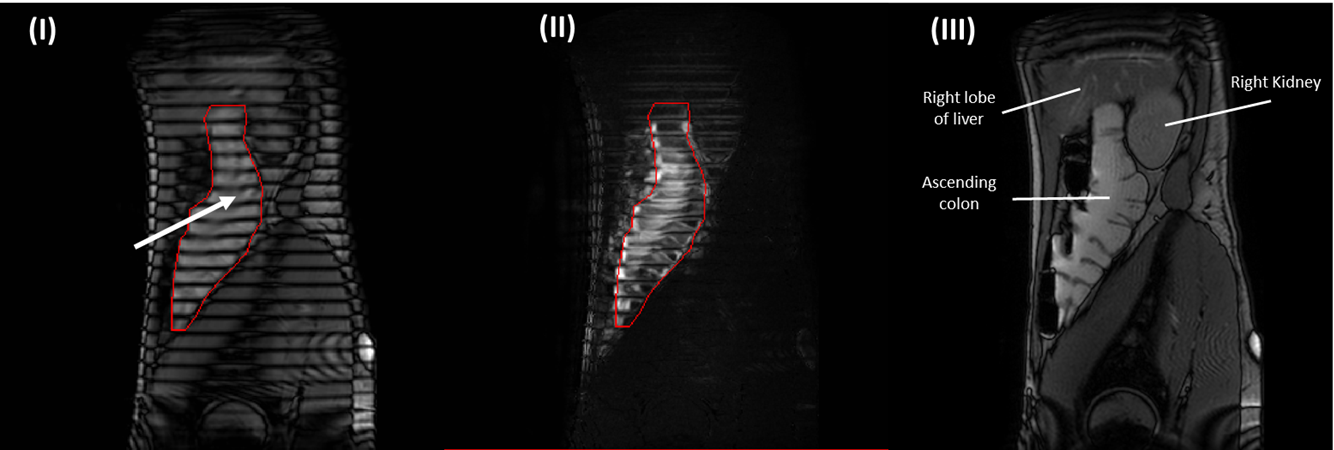
Figure 2: The generated maps of the ascending colon after applying the tagging (dark horizontal stripes across the image), (i) Mean pixel intensity map, (ii) Corresponding pixel standard deviation (std dev) map, and (iii) high resolution T2 image (sagittal oblique) with anatomical labels. A visible small motion of colonic contents is highlighted (white arrow) which is indicated by the tags distortion. Colon regions (ROIs) are outlined in red.
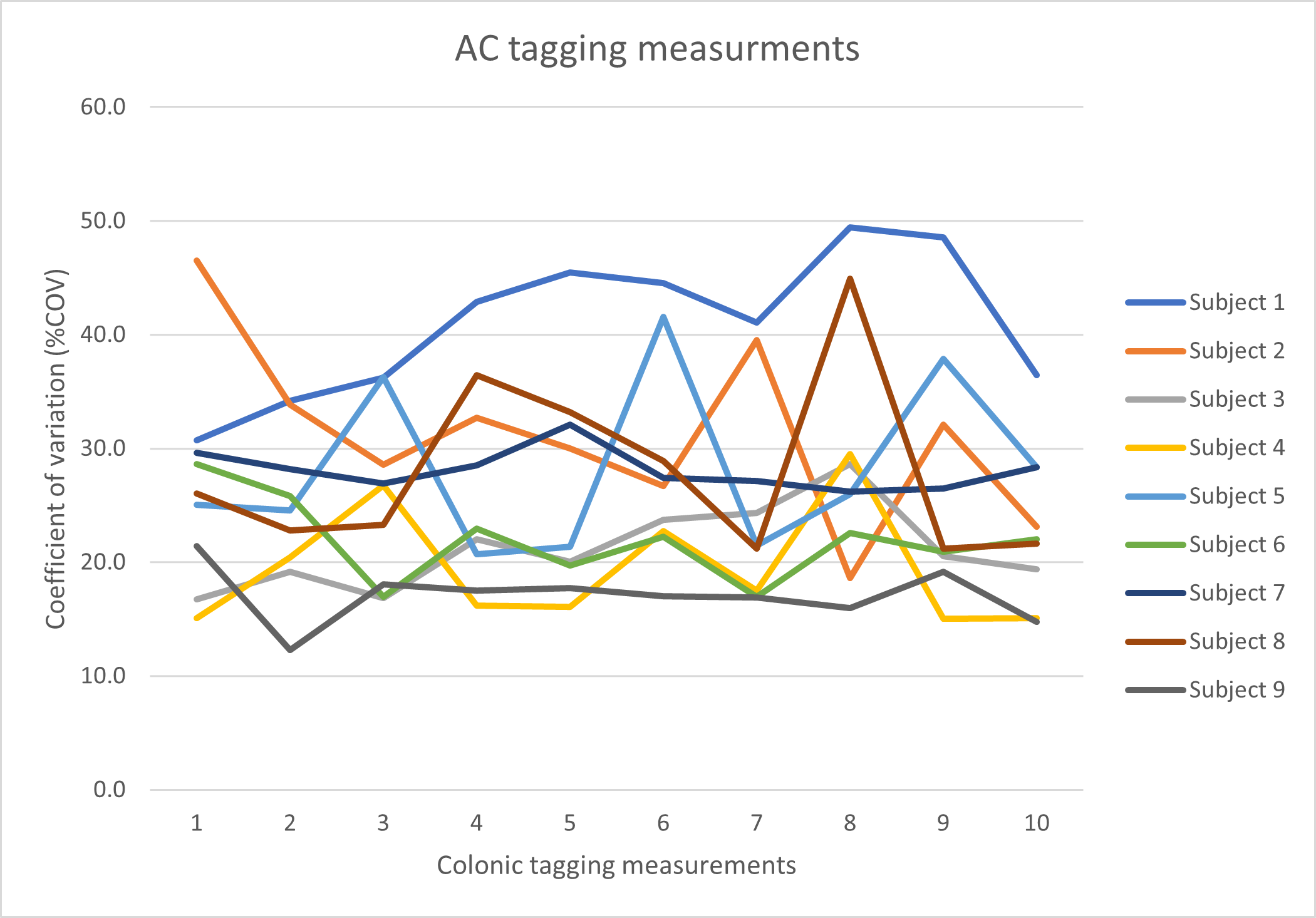
Figure 3: The change over time between the multiple scans for the ascending colon.
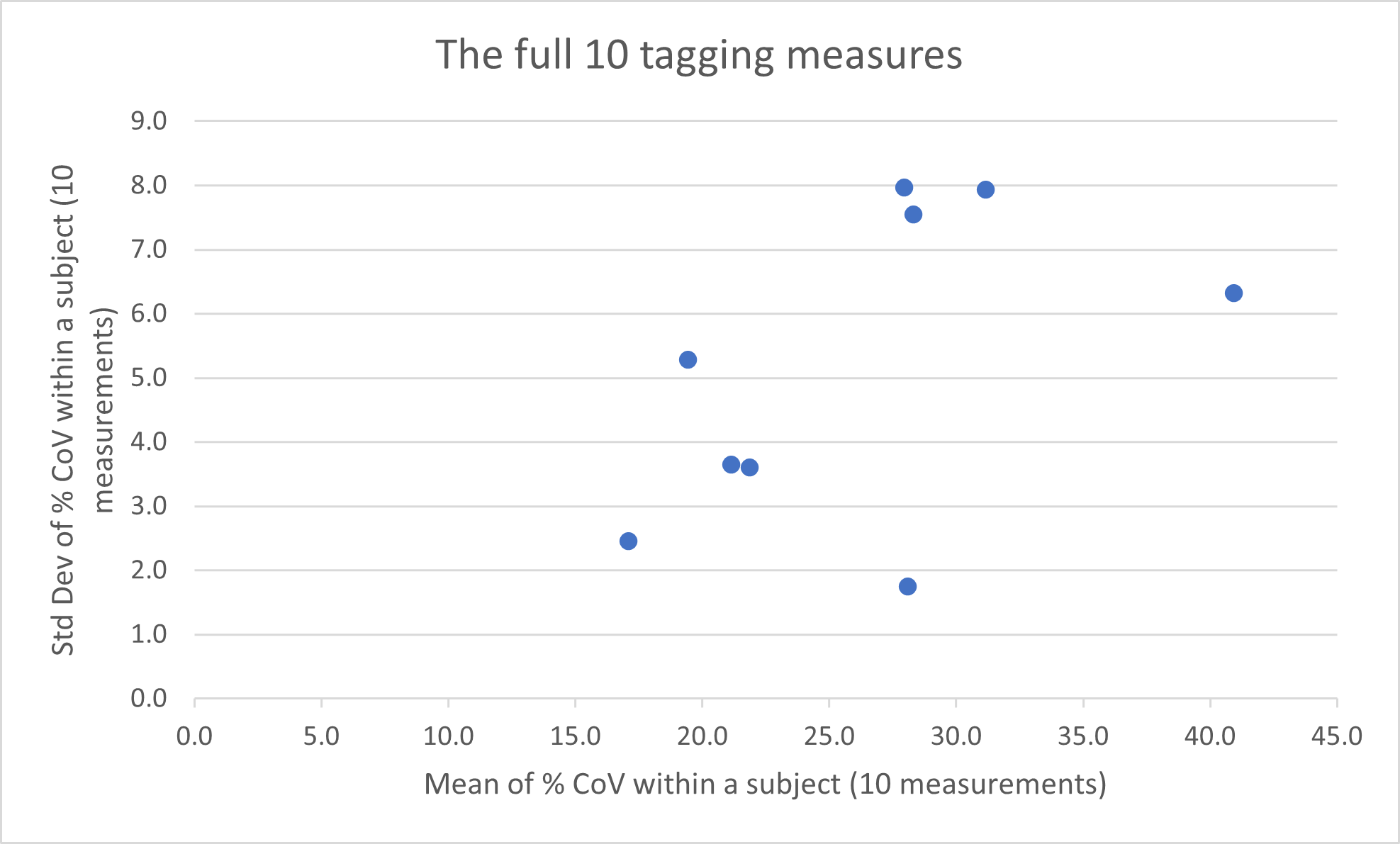
Figure 4: Mean and standard deviation (std dev) of coefficient of variation (%COV) for each subject (within subject) of all the scans.
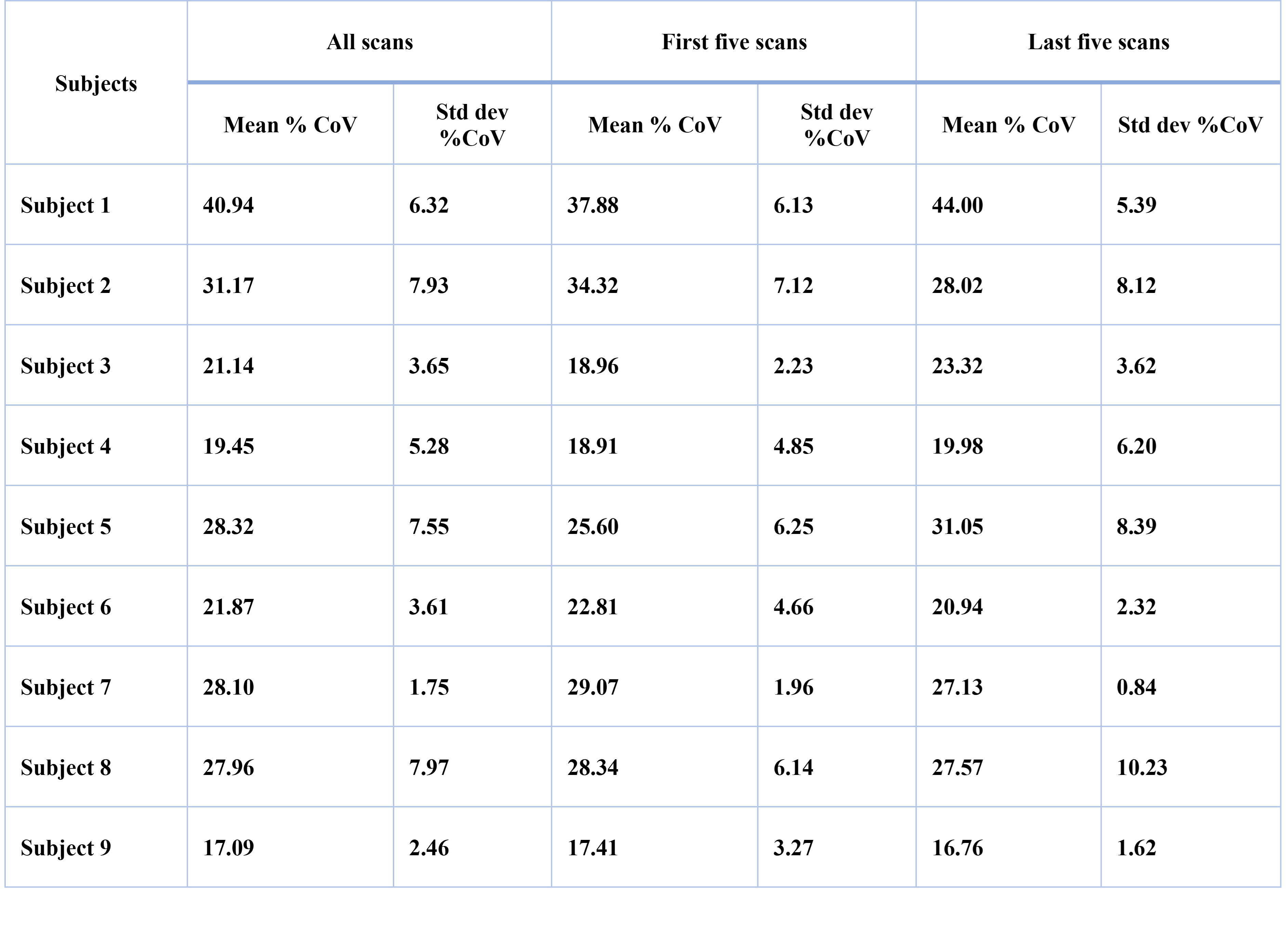
Table 1: Mean and standard deviation (std dev) of %COV for each subject of all the scans, first scans, and last five scans, respectively.