2039
The feasibility of DCE-MRI in presurgical evaluation of tumor budding grade in rectal cancer1Department of Radiology, the First Affiliated Hospital of Dalian Medical University, Dalian, China, 2The First Affiliated Hospital of Dalian Medical University, Dalian, China
Synopsis
Tumor budding (TB) is a histopathologic characteristic which has led to a growing interest in the prognosis prediction of cancers of various sites. Preoperative prediction of TB status may help personalize treatment in rectal cancer cancer patients. Previous studies showed MRI-based and PET/CT based radiomics can predict TB status, however, the high cost and complex post-processing limit their clinical applications. Dynamic contrast-enhanced (DCE) MRI has been extensively evaluated aggressiveness of rectal cancer. Results of this study indicate Kep values can effectively differentiate high from intermediate-low grade TB.
Introduction
Tumor budding (TB) is defined as a single neoplastic cell or cell cluster of up to four neoplastic cells at the invasive front of the tumor or within the tumor mass 1. Compared to intermediate-low grade TB(0–9 buds), High grade TB (10 or more buds) are associated with higher risk of lymph node metastasis, recurrence and mortality2. A preoperative imaging study which can predict TB grade reliably is urgent. However, there are few studies on the imaging manifestations of TB and radiomics adopted by previous studies is too complicated to apply to clinical work3. Dynamic contrast-enhanced (DCE) MRI is a functional imaging that can provide valuable information about tumour aggressiveness and the degree of angiogenesis. The purpose of this study is to explore the value of DCE-MRI in predicting TB grade of rectal cancer.Methods
This study has been approved by the local IRB. 25 patients with pathologically confirmed with rectal cancer were recruited in this study. The patients were divided into two groups: intermediate-low grade TB group (19 patients) and high grade TB (6 patients) groups. They underwent a examination on 3.0T MR (Signa HDxt, GE Medical Systems, USA) with a phased-array body coil. The MR sequences included T2WI, DWI LAVA, etc. Detailed parameters were listed in Table 1. Ktrans, Kep and Ve maps were calculated from DCE by using GenIQ software at ADW 4.6 workstation. Two radiologists used a double-blind method to place three ROIs on the largest layer of the lesion to measure DCE parameters. The average values were calculated to minimize measurement bias. An unpaired t-test was used to analyze the differences of DCE parameters between the two groups, and the ROC curves were used to evaluate the diagnostic efficacy of these parameters in predicting TB grade of rectal cancer.Results
The consistency of the data obtained by the two observers was good (ICC value > 0. 75). The Kep values of intermediate-low TB grade group were significantly higher than those of high grade TB group (P<0.05). No significant difference of Ktrans and Ve values was observed between the two groups (P>0.05). The AUC values for the ROC analyses of Kep values for differentiation between high and intermediate-low TB grade groups was 0.88. When setting the threshold of Kep value to be 1.6/min, the corresponding diagnostic sensitivity and specificity would be 100 and 73.7.Discussion and Conclusion
The Kep values of high grade TB group were significantly smaller than those of intermediate-low TB grade, which contradict some previous studies about DCE-MRI4. This may be due to stromal invasion of TB. Kep represents the efflux rate of gadolinium contrast from the extracellular extravascular space back into plasma.The interstitial space of rectal cancer with high grade TB is largely occupied by neoplastic cell cluster, makes it more difficult for the contrast agent to leak into the tumor tissue. In summary, DCE parameters may serve as a promising tool for clinical differentiation of TB grade in rectal cancer.Acknowledgements
No acknowledgement found.References
1. Koelzer VH, Zlobec I, Lugli A. Tumor budding in colorectal cancer--ready for diagnostic practice?. Hum Pathol. 2016;47(1):4-19.
2. Ueno H, Mochizuki H, Shinto E, et al. Histologic indices in biopsy specimens for estimating the probability of extended local spread in patients with rectal carcinoma. Cancer, 2002, 94(11): 2882-2891.
3. Li Z, Chen F, Zhang S, et al. The feasibility of MRI-based radiomics model in presurgical evaluation of tumor budding in locally advanced rectal cancer [published online ahead of print, 2021 Oct 21]. Abdom Radiol (NY). 2021;10.1007/s00261-021-03311-5.
4. Dijkhoff RAP, Beets-Tan RGH, Lambregts DMJ, Beets GL, Maas M. Value of DCE-MRI for staging and response evaluation in rectal cancer: A systematic review. Eur J Radiol. 2017;95:155-168.
Figures
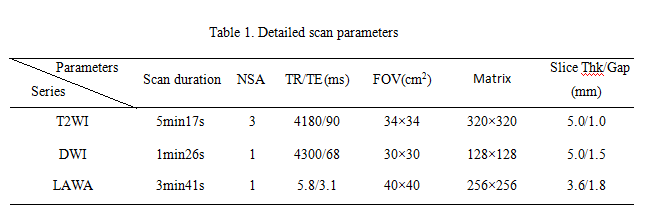
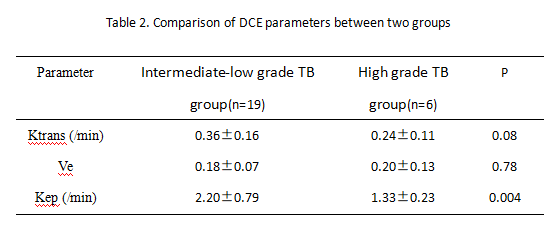
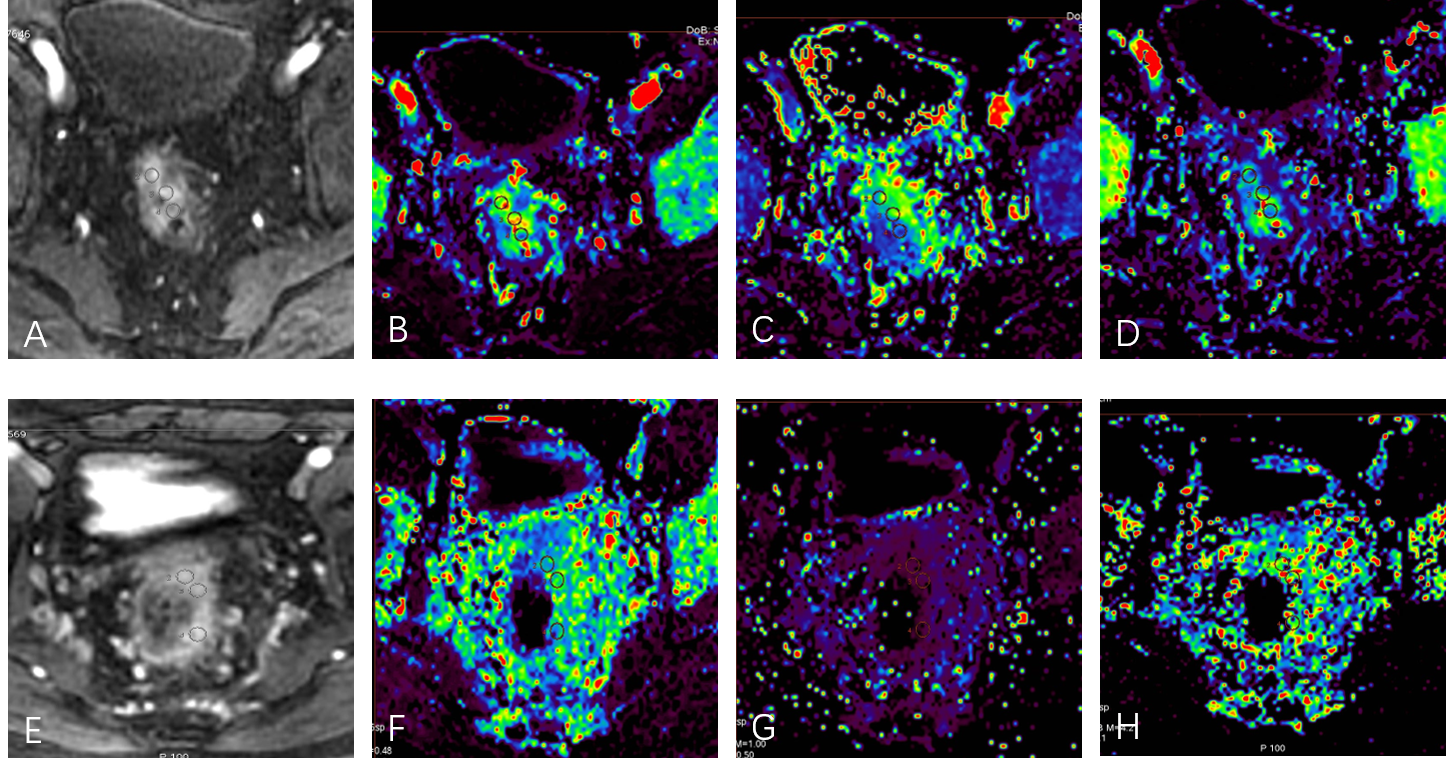
Figure 1. A 66-year-old male, rectal cancer with high grade TB . The LAVA(A), Ktrans (B), Ve(C), Kep (D) maps were shown, Ktrans , Ve, Kep values are 0.285/min, 0.258, 1.17/min,respectively.
A 54-year-old male, rectal cancer with low grade TB . The LAVA(E), Ktrans (F), Ve(G), Kep (H) maps were shown, Ktrans , Ve, Kep values are 0.157/min, 0.057, 2.16/min,respectively.