2035
Pancreatic iron is a marker of cardiovascular complications in sickle cell disease1Fondazione G. Monasterio CNR-Regione Toscana, Pisa, Italy, 2Gemelli Molise SpA, Fondazione di Ricerca e Cura "Giovanni Paolo II", Campobasso, Italy, 3Ospedale del Delta, Lagosanto (FE), Italy, 4Azienda Ospedaliera "Garibaldi" Presidio Ospedaliero Nesima, Catania, Italy, 5Ospedale “SS. Annunziata” ASL Taranto, Taranto, Italy, 6Policlinico "G. Martino", Messina, Italy, 7Azienda Ospedaliero Universitaria Pisana, Pisa, Italy, 8Azienda Ospedaliero - Universitaria Careggi, Firenze, Italy
Synopsis
We systematically explored the link between pancreatic iron detected by the T2* Magnetic Resonance Imaging technique and cardiovascular complications in a cohort of 63 patients with sickle cell disease (SCD). Patients with cardiovascular complications (supraventricular arrhythmias, heart failure, pulmonary hypertension, myocardial infarction, deep vein thrombosis, leg ulcers) showed significantly lower global pancreas T2* values than patients free of cardiovascular complications but comparable global heart T2* values. Pancreatic iron overload (T2*<26 ms) was associated with 7.5 times higher odds of cardiovascular complications.
Introduction
A strong association between pancreatic iron burden and cardiac complications was found in patients with thalassemia major1. There is no study evaluating this issue in sickle cell disease (SCD).The objective of this multicenter study was to systematically explore the link between pancreatic iron and cardiovascular complications in a cohort SCD patients enrolled at baseline in the prospective Extension-Myocardial Iron Overload in Thalassaemia (E-MIOT) project.
Methods
We considered consecutively enrolled 63 patients: 44 with sickle beta thalassemia, 18 with sickle cell anemia (SCA), and one with hemoglobin SC disease (HbSC). Mean age was 36.6±14.4 years and 29 patients were females.T2* measurements were performed over pancreatic head, body and tail and global value was the mean2,3. Myocardial iron overload (MIO) was quantified using a T2* segmental approach4.
Results
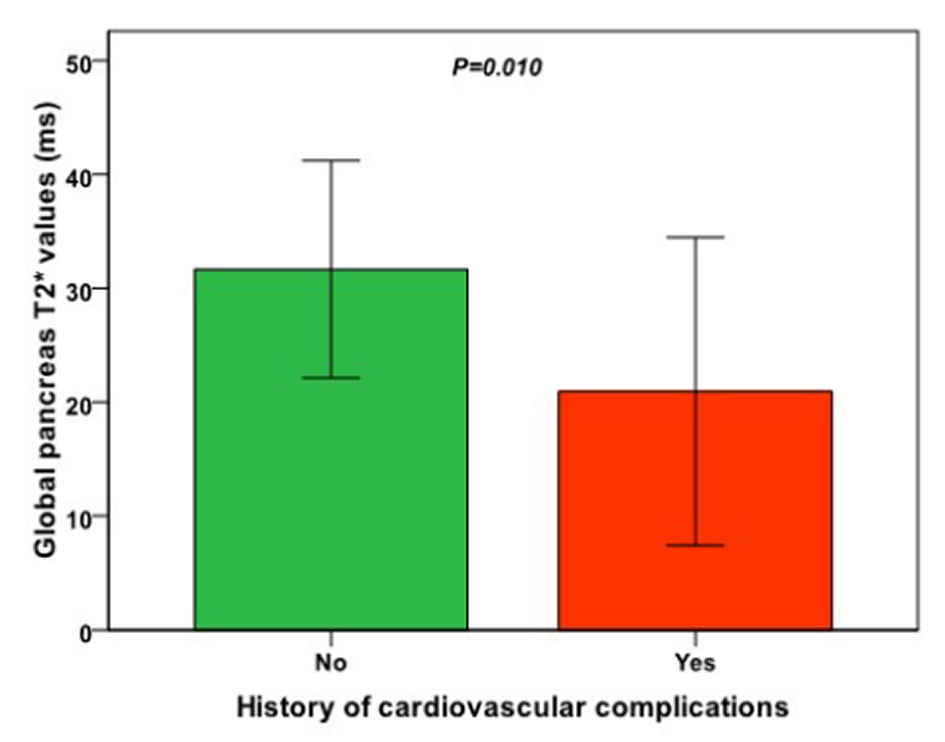
SCA and sickle beta thalassemia patients were comparable for age, sex, hematochemical parameters, and cardiac and pancreatic T2* values. Transfusion dependent (TD; N=44) and no-TD patients showed comparable global pancreas T2* values (29.8±11.4 ms vs 32.2±8.0 ms; P=0.414), but were more frequently chelated (79.1% vs 52.6%; P=0.034). Nineteen patients (30.2%) showed a pathological global pancreas T2* value (<26 ms) while no patient had significant myocardial iron overload (global heart T2*<20 ms).Seven patients (11.1%) had at least one cardiovascular complication: two supraventricular arrhythmias, one heart failure, one heart failure + pulmonary hypertension, one myocardial infarction, one deep vein thrombosis, and one leg ulcer. Frequency of cardiovascular complications was comparable among the forms of SCD, but all complications occurred in regularly transfused patients. Patients with cardiovascular complications showed significantly lower global pancreas T2* values than patients free of cardiovascular complications (20.9±13.5 ms vs 31.7±9.6 ms; P=0.010) (Figure 1) but comparable global heart T2* values (38.4±5.6 ms vs 40.6±4.7 ms; P=0.257). Patients with pancreatic iron overload were more likely to have cardiovascular complications [odds ratio=7.5 (95%confidence intervals=1.3-43.1); P=0.024].
Conclusions
Pancreatic iron overload is associated with an increased risk of cardiovascular complications in SCD patients. If a patient has pancreatic iron overload, it would be prudent to start or intensify iron chelation therapy to prospectively prevent cardiac damage.Acknowledgements
We would like to thank all the colleagues involved in the E-MIOT project (https://emiot.ftgm.it/) and all patients for their cooperation.References
1. Pepe A, Pistoia L, Gamberini MR, et al. The Close Link of Pancreatic Iron With Glucose Metabolism and With Cardiac Complications in Thalassemia Major: A Large, Multicenter Observational Study. Diabetes Care. 2020;43(11):2830-2839.
2. Restaino G, Meloni A, Positano V, et al. Regional and global pancreatic T*(2) MRI for iron overload assessment in a large cohort of healthy subjects: Normal values and correlation with age and gender. Magn Reson Med. 2011;65(3):764-769.
3. Meloni A, De Marchi D, Positano V, et al. Accurate estimate of pancreatic T2* values: how to deal with fat infiltration. Abdom Imaging. 2015;40(8):3129-3136.
4. Meloni A, Positano V, Pepe A, et al. Preferential patterns of myocardial iron overload by multislice multiecho T*2 CMR in thalassemia major patients. Magn Reson Med. 2010;64(1):211-219.
Figures