2004
A Wireless Pilot Tone Based Patient Squeeze-Ball (P2TSB)1MR R&D CFP, Siemens Healthineers, Erlangen, Germany, 2MR DL CARD, Siemens Healthineers, Erlangen, Germany, 3MR R&D HW&SYS CRX, Siemens Healthineers, Erlangen, Germany
Synopsis
We developed a prototype wireless patient alarm-ball based on Pilot Tone technology which could speed up patient setup time and increase patient comfort. The use of Pilot Tone as a means of signal transmission enables easy and cost-effective use of this concept on existing scanners with only a minimal software upgrade.
Motivation
The squeeze-ball is a signaling device used by the patient inside an MRI scanner to notify the operator, located outside the scan room, when direct communication is not possible because of the high noise level during an MRI exam. It comprises of a small rubber ball that fits into the patients hand and is usually connected through a rubber hose to a pressure sensitive switch. When pressed, an alarm is raised at the operator’s console. However, the long hose can easily be tangled up with other wired equipment, such as headphones, coil cables, ECG leads etc., increasing patient discomfort and making patient preparation more complicated. Here, we propose to replace the current solution with a battery powered, wireless unit where transmission of the activation signal is piggybacked onto the Pilot Tone[1] system previously proposed for physiological monitoring – the Pilot Tone Patient Squeeze Ball (P2TSB).Methods
A prototype P2TSB transmitter was developed in-house, comprising of a rubber ball connected to a pressure sensitive switch and a free running oscillator running at f=62.5MHz (Figure 1, 2). When the ball is pressed, a continuous wave signal is generated and received by all active local coil elements simultaneously[2]. The signal is run continuously over a certain period of time, e.g. tactivation,min = 1s, to ensure that the detection is not hindered by a RF pulse transmitted at the same time.For signal detection, we use our in-house developed PT processing framework to continuously monitor (fsample = 2kHz) the sliding variance and amplitude in the 62.5MHz frequency band. We differentiate between four possible use scenarios:
1. No active PT source is present, i.e. PT is not used for physiological monitoring
- a) Not scanning – no active RF pulses
- b) Scanning – some sample points are masked due to active RF pulses
2. Active PT source is present, i.e. PT is used for physiological monitoring
- a) Not scanning – no active RF pulses
- b) Scanning – some sample points are masked due to active RF pulses
In scenarios 1a and 1b, no active PT source is present and thus modulation from physiological motion is not considered.
In scenarios 2a and 2b, PT is used for physiological monitoring and thus an active PT signal is being generated and modulated by physiological motion.
In scenarios 1b and 2b, RF pulses are being played out and reception is blanked in order to safeguard the receive circuitry. Thus, some samples are masked and must not be considered in the determination of variance.
We chose a window length of twin = 50-100 valid samples for the sliding variance filter to ensure a) that even with active scanning, enough valid sample points are being recorded and b) the variance is affected mainly by the activation of the additional squeeze-ball PT signal and not by physiological motion modulation, if present.
Results
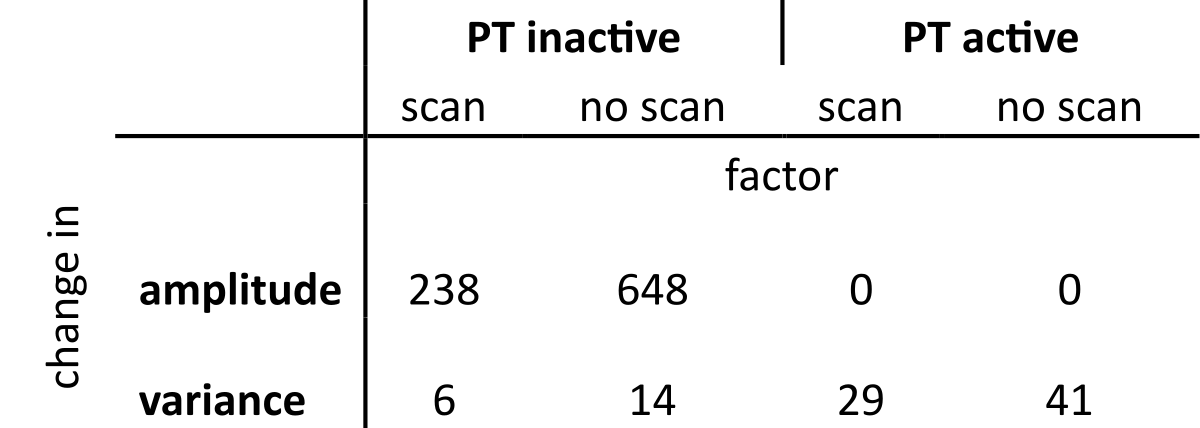
Figure 3 shows the raw PT signal of one representative channel for scenarios 1 and 2 (left) as well as the output of the sliding variance filter (right). Samples that have been masked out due to active RF have been removed and periods with RF (scanning) are depicted by a red bar. Periods of squeeze-ball activation are indicated by green bars.We found that activation of the squeeze-ball results in an increase of variance in all scenarios, while the mean of the signal changes only in scenario 1. In this case, no active PT signal is present and data recorded at this frequency is zero plus noise. When the ball is active, it constitutes an active PT source and the signal amplitude changes significantly (see Table 1).
Note that during scanning, both variance and mean are changed due to residual RF signal components in the PT frequency band. This also results in a short spike in sliding variance (red arrows in Fig. 3, panel 2). However, these spikes are of very short duration and can be disregarded easily as they do not fulfill the minimum duration requirement tactivation,min for squeeze-ball activation.
Summary and Outlook
The proposed PT based wireless squeeze-ball is an attractive concept as it is easy to implement and, as the reception of the signal is done by the existing receiver hardware, even existing scanners can be retrofitted to support it with only a minor software update. Since the squeeze-ball is activated in emergency situations only, there is no risk of generating MR image artifacts. Also, no RF spectrum is blocked. Since the energy requirements of this device are minimal, it could be powered using supercapacitors, ensuring sufficient charge for at least one day of use while also enabling rapid charging.Detection of squeeze-ball activation by monitoring the sliding variance is straightforward, with clear changes in variance being observed in all use scenarios and requirements on processing power are negligible. When no active PT source is present, simply monitoring the amplitude in the PT signal band is sufficient to detect activation.
If PT is used for physio monitoring, some degradation of the PT physio signal during squeeze-ball activation is to be expected, but since the squeeze-ball is activated in emergency situations only, this is of little consequence.
Acknowledgements
No acknowledgement found.References
[1] Speier P, Fenchel M, Rehner R. PT-Nav: a novel respiratory navigation method for continuous acquisitions based on modulation of a pilot tone in the MR-receiver. In: Magnetic Resonance Materials in Physics, Biology and Medicine. Vol. 28. ; 2015. pp. 97–98. doi: 10.1007/s10334-015-0487-2.
[2] Bacher M, Dornberger B, Bollenbeck J, Stuber M, Speier P. Listening in on the Pilot Tone: A Simulation Study. In: Joint Annual Meeting of the ISMRM & ESMRMB, Virtual. ; 2021. p. 1364.
Figures
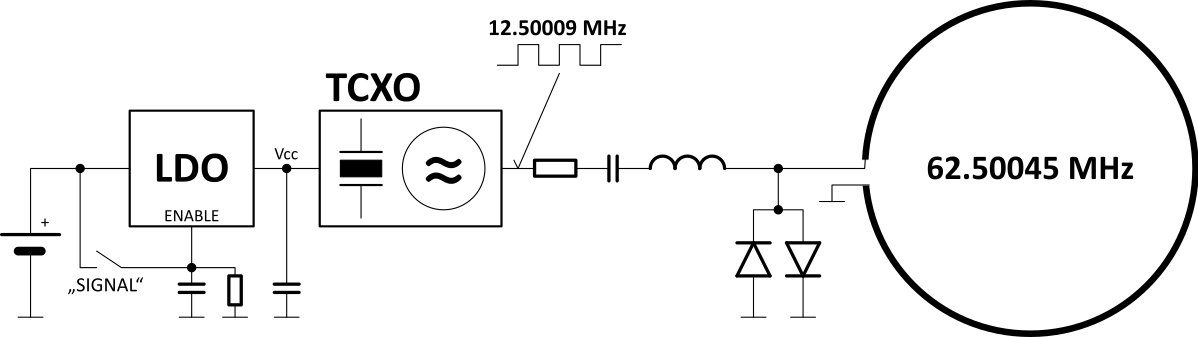
Figure 1: Schematic of the prototype wireless squeeze-ball. A pressure sensitive switch (“Signal”) is connected to a free running oscillator, generating a continuous wave signal at f=62.5MHz upon activation which couples inductively to the scanners receive coils.
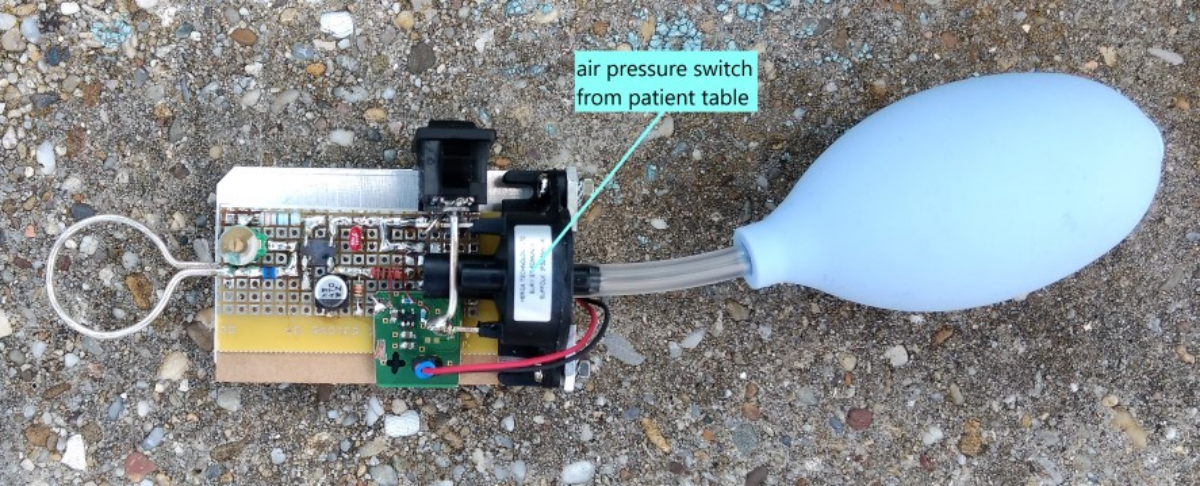
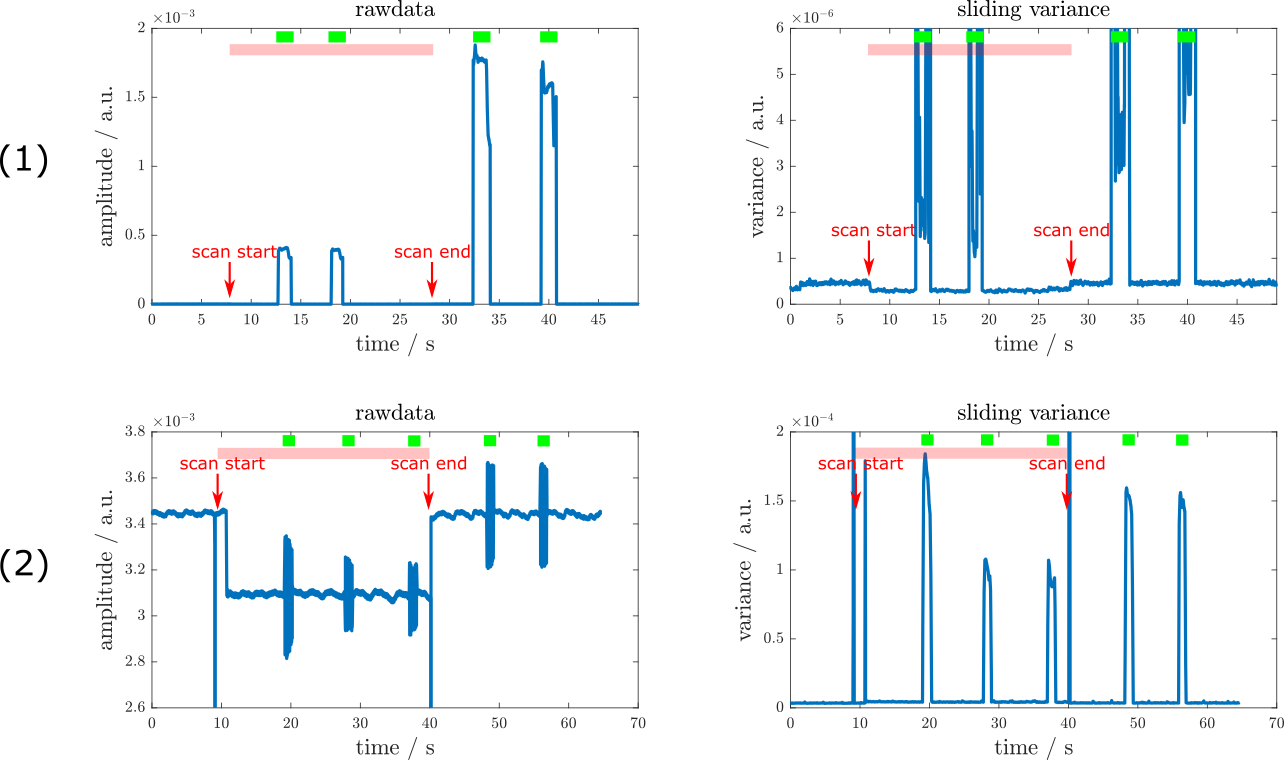
Figure 3: Raw data (left) and sliding variance (right) in scenarios 1 (top) and 2 (bottom). Periods of scanning are indicated by a red bar. Green bars denote squeeze-ball activations. The start and end of the scan are indicated by red arrows. In the raw signal of scenario 2, the modulation of the PT signal by physiological motion can be clearly observed.