1969
Retrospective correction of B1 field inhomogeneities in T2w 7T prostate patient data
Seb Harrevelt1, Daan Reesink2, Astrid Lier, van3, Richard Meijer3, Josien Pluim4, and Alexander Raaijmakers1
1TU Eindhoven, Utrecht, Netherlands, 2Meander Medisch Centrum, Utrecht, Netherlands, 3UMC Utrecht, Utrecht, Netherlands, 4TU Eindhoven, Eindhoven, Netherlands
1TU Eindhoven, Utrecht, Netherlands, 2Meander Medisch Centrum, Utrecht, Netherlands, 3UMC Utrecht, Utrecht, Netherlands, 4TU Eindhoven, Eindhoven, Netherlands
Synopsis
Prostate imaging at ultra-high fields is heavily affected by B1 field induced inhomogeneities. This not only results in unattractive images but it also might affect clinical diagnosis . To remedy this we developed a deep learning model that retrospectively corrects for the bias field. We applied this model to a clinical data set and demonstrated its performance in a qualitative manner. The results indicate that the model is able to drastically reduce the inhomogeneities in a variety of cases while the tissue contrast is generally maintained and the underlying anatomy has been successfully recovered.
Introduction
T2w prostate imaging at 7T has potential for clinical purposes because of its superior resolution and enhanced tissue contrast. In addition, the modality is indispensable for lesion localization in (X-nuclei) MR spectroscopy. However, the images suffer from B1 field induced inhomogeneities. B1 shimming1 , TIAMO2 and parallel transmit3 are techniques that can reduce but not avoid these inhomogeneities. Although the imaging target can be clearly depicted, the surrounding signal voids and overall transmit and receive field inhomogeneity clearly reduce the attractiveness for clinical users. In addition, inhomogeneities may hinder the detection of anomalies and automatic image post processing methods such as segmentation become more difficult4,5. Reduction of these inhomogeneities is expected to improve usability and facilitate the adoption of 7T for clinical body imaging applications. For this purpose, we present a deep-learning approach to retrospectively correct 7T prostate images to alleviate the B1-field induced signal inhomogeneities. This work is a continuation of previous work where a neural network was trained to correct multi channel acquisitions of inhomogenous prostate images6. With the current extension we enable retrospective application on existing clinical data sets. The performance of this approach is tested on T2w 7T images from 14 prostate cancer patients.Methods
We consider the 7T image as the product of the underlying homogeneous image and a distribution of B1-field induced inhomogeneities, which we call the bias field. The method was developed for prostate images obtained with a transmit-receive array of eight fractionated dipole antennas7. We have created a training data set that mimics T2w prostate images at 7T using homogeneous clinical prostate images at 1.5T and simulated B1 field distributions at the 7T Larmor frequency, see Figure 1. A ResNet architecture and a Perceptual Style Loss were used for training, where the goal of the training was to predict the bias field from the artificial 7T input image. To obtain a bias field corrected image during inference we divide the input image by the predicted bias field from the trained neural network. This approach was preferred over predicting a homogeneous image directly to avoid that the network would be trained to fill signal voids with ‘invented’ tissue structures. The trained network was applied retrospectively to T2w 7T images of 14 prostate cancer patients (age 48-72). The TSE acquisition was obtained with an RF coil array setup with eight transmit/receive fractionated dipole antennas and sixteen receive-only loop coils. A repetition time of 10s, and a TE of 140ms was used with a reconstructed pixel size of 0.28x0.28x3mm.Results
Figure 2 displays the original and corrected images. Generally speaking, the corrected images from the deep learning model show a drastic decrease of inhomogeneity without significantly altering the contrast between fat- and muscle tissue, or of the prostate tissue itself. In mild cases, such as example 1, 5, 8 and 9, we notice an almost complete removal of the bias field and recovery of the underlying anatomy. Whereas more severe cases, where RF shimming was performed poorly such as example 11, 12 and 13, the model has difficulty in recovering the underlying anatomy and returns noise instead. In Figure 3 we present a close-up of the same images to accurately asses the quality of the biasfield reduction around the prostate. Here we notice that in example 2, 4, 6, 12, and 14 our method is able to recover obscured parts of the peripheral which is important for asessment of extraprostatic extension. Moreover, in example 2, 4, 6, 7 and 14 we see a great enhancement of the edges at the rectum wall, although sometimes these enhancements are accompanied by an overcompensation resulting in bright regions inside the rectum.Discussion
The proposed method clearly improves the prostate images. B1-field induced inhomogeneities in signal intensity are removed almost completely. Please note that the method only corrects for global signal inhomogeneity but does not restore loss of local contrast because of suboptimal flip angles. As expected, the choice for the bias field as network output ensures that areas with low signal intensity have been corrected by noise amplification and not by a plausible but imaginary anatomy structure. In addition, in most cases the model does not affect tissue contrast however sometimes it does enhance the contrast of the prostate tissue as shown in example 4, 8 and 13. Remarkably, these patient images were acquired with a 24 element receive array while the method was trained on 8-channel receive fields, which apparently does not affect the performance. Note that the images were acquired in a realistic clinical work flow which sometimes resulted in suboptimal B1 shimming, e.g. 10, 11 and 12. Future work will investigate the apparent improvement in clinical usability by expert rating.Conclusion
We have developed a method that is able to retrospectively correct the B1-field induced inhomogeneities in T2w prostate images at 7T. The model was trained on an artificial 7T data set by combining a set of clinical T2w 1.5T prostate images with simulated B1 field distributions at 7T. The model was tested using T2w 7T images from 14 prostate cancer patients. Corrected images are drastically improved with much less signal inhomogeneities while signal contrast throughout the image is preserved.Acknowledgements
No acknowledgement found.References
1. Roemer, Peter B., et al. "The NMR phased array." Magnetic resonance in medicine 16.2 (1990): 192-225. 2 Orzada, Stephan, et al. "RF excitation using time interleaved acquisition of modes (TIAMO) to address B1 inhomogeneity in high‐field MRI." Magnetic Resonance in Medicine 64.2 (2010): 327-333. 3 Rietsch, Stefan HG, et al. "Parallel transmit capability of various RF transmit elements and arrays at 7T MRI." Magnetic resonance in medicine 79.2 (2018): 1116-1126. 4. Chen, Jingyun, Louisa Bokacheva, and Henry Rusinek. "Image Segmentation and Nonuniformity Correction Methods." 3D Printing for the Radiologist. Elsevier, 2022. 31-43. 5. Despotović, Ivana, Bart Goossens, and Wilfried Philips. "MRI segmentation of the human brain: challenges, methods, and applications." Computational and mathematical methods in medicine 2015 (2015). 6. S. Harrevelt, L. Wildenberg, D. Klomp, C.A.T. van den Berg, Josien Pluim, and Alexander Raaijmakers. “Reduction of B1-field induced inhomogeneity for body imaging at 7T using deep learning and synthetic training data.”. ISMRM 2021 (2021) 7 Raaijmakers, Alexander JE, et al. "The fractionated dipole antenna: A new antenna for body imaging at 7 T esla." Magnetic resonance in medicine 75.3 (2016): 1366-1374Figures
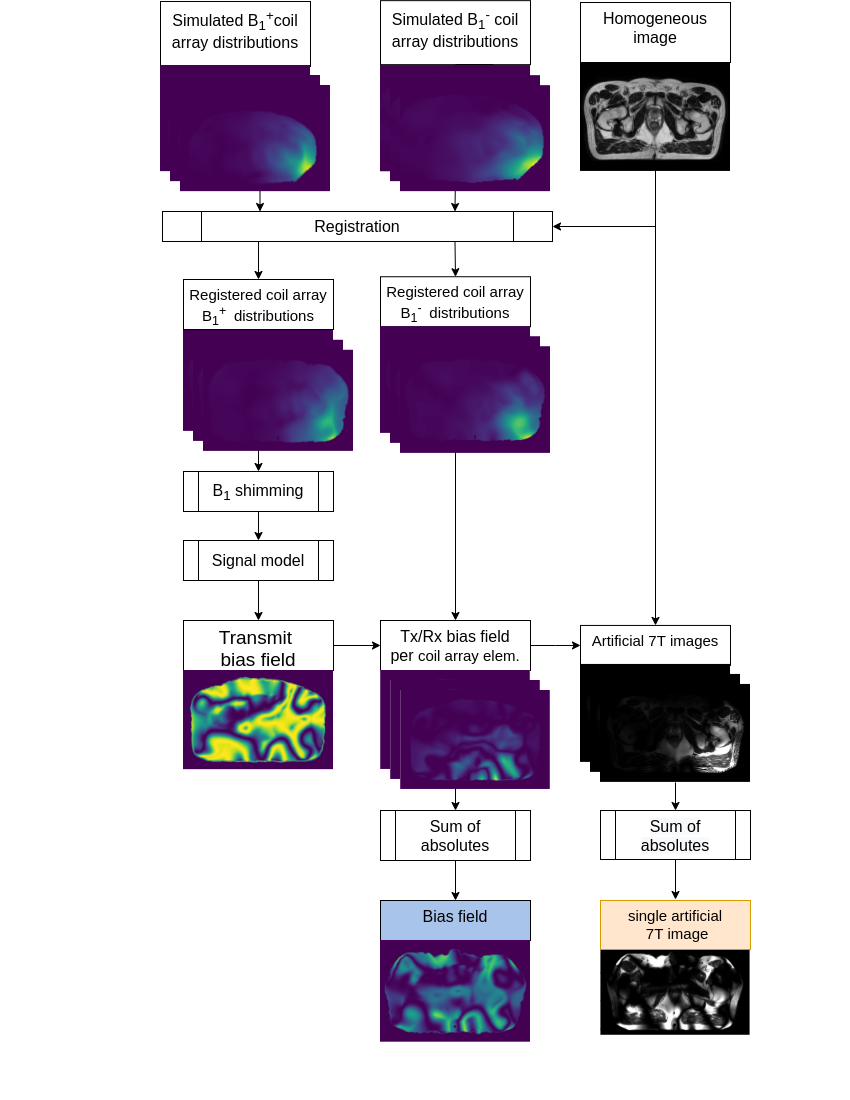
Representation of the pipeline for creating
artificial training data. Simulated 7T B1 fields of the coil array
are registered to the body contour of the 1.5T prostate image,
followed by a RF shimming routine on the B1+ coil distributions. The obtained transmit field is input to a signal model
to imitate the signal of a TSE scan. By multiplying the obtained
signal with the registered B1- fields we
obtained the bias field per coil. The image under the blue colored box is used as target, and the image under the orange colored box is used as input for the deep
learning model.
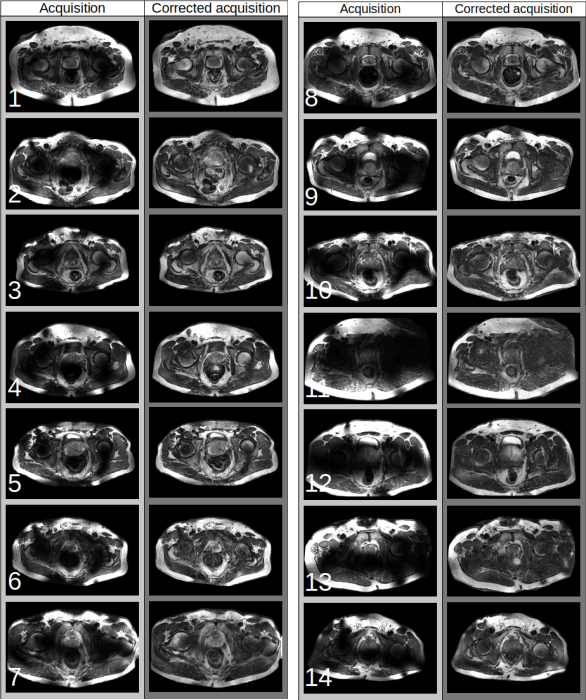
Results of the B1 field inhomogeneity correction on T2w 7T images of
14 prostate cancer patients. Figure presents images as obtained from the
scanner accompanied by the corrected images. For each patient, only the
center slice was depicted to demonstrate the performance of our model.
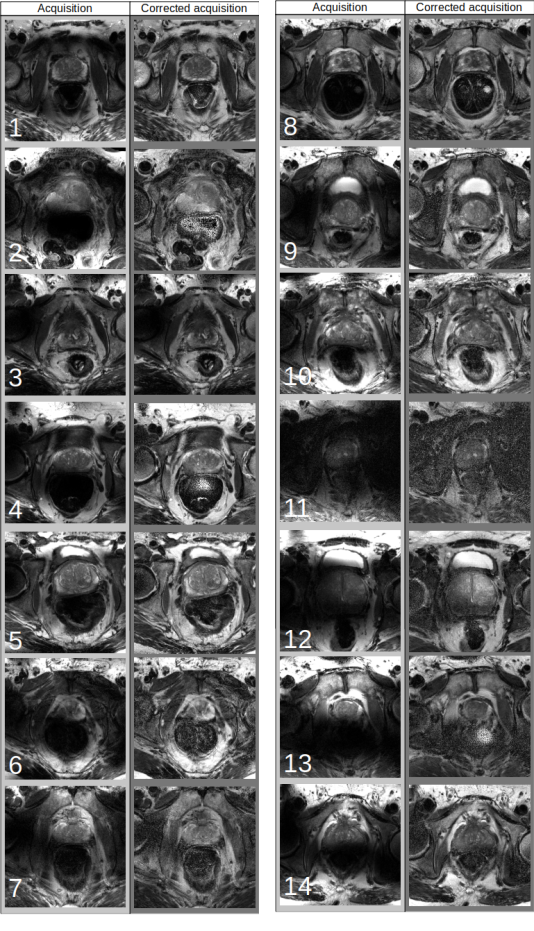
Close up of the images as presented in Figure 2. This view enables more close examination of the performance of the model in the periphery of the prostate and the internal tissue structures of the prostate.
Animated representation of inhomogeneity correction over all slices of two selected patients.
DOI: https://doi.org/10.58530/2022/1969