1928
Structural Connectivity in Default Mode Network May Lateralize Temporal Lobe Epilepsy: A Graph-Theory Approach1Medical Physics and Biomedical Engineering, Tehran University of Medical Sciences, Tehran, Iran (Islamic Republic of), 2Research Center for Molecular and Cellular Imaging, Tehran University of Medical Sciences, Tehran, Iran (Islamic Republic of), 3Biomedical Engineering, Hamedan University of Technology, Hamedan, Iran (Islamic Republic of), 4Medical School, Tehran University of Medical Sciences, Tehran, Iran (Islamic Republic of)
Synopsis
Difficulties in lateralizing the epileptogenic side of the brain challenge the temporal lobe epilepsy (TLE) surgery. We examined structural connectivity in default mode network (DMN) based on graph network analysis for specifying the epileptogenic side of the brain in TLE patients. The results showed significantly different connectivity in DMN nodes among the TLE patients compared to the control cohort. DMN regions with abnormal structural connectivity in TLE subjects corresponded with the epileptogenic brain sides.
Introduction
Temporal lobe epilepsy (TLE) is the most frequent type of localized epilepsy in adults, covering 60 to 75% of surgeries in patients with drug-resistant epilepsy [1]. Difficulties in determining the epileptogenic side of the brain impose challenges in the resective surgery of associated temporal structures. The TLE has been found to affect many brain networks, including Default Mode Network (DMN) [2]. We investigated structural connectivity in DMN based on a graph theory approach, in order to identify the epileptogenic side of the brain in TLE patients.Methods
We recruited 35 patients (21 Left-TLE and 14 Right-TLE) and 20 healthy subjects as a control (HC) cohort with the data acquisition on a Siemens Magnetom Prisma 3T MRI system. The diffusion imaging protocol consisted of a single diffusion shell (1000 s/) of 64 volumes for each diffusion-gradient direction, and 5 reference volumes for null diffusion gradient (b0 s/) with voxel size of 2×2×2 , TR/TE of 9600/92 ms. A reversed-phase encoding was additionally acquired for distortion correction of diffusion images. A high resolution T1 anatomical image was acquired for each case using the 3D magnetization-prepared rapid gradient echo sequence (MPRAGE) with voxel size of 1.1×1.1×1.0 , TR/TE of 1840/2.43 ms, and flip angle of 8֠. The data were processed using the MRtrix3 software package (http://www.mrtrix.org). The diffusion data was processed through the entire pre-processing pipeline including denoising, Gibb’s ringing removal, geometric distortion correction, and bias-field correction. The multi-shell multi-tissue algorithm of constrained spherical deconvolution (CSD) [3] was applied for modeling the cerebrospinal fluid and white matter compartments with a maximum spherical harmonic order (Lmax) of 8. Following the initial processing, connectomes were generated and tractogram was subsequently constructed with 35 million probabilistic streamlines generation using the 2nd -order integration over the Fibre Orientation Distributions algorithm (iFOD2)3 and anatomically-constrained tractography (ACT) [4]. Using spherical-deconvolution informed filtering of tractograms (SIFT) [5], a weight was assigned to each streamline, to make the measurement of connectivity biologically meaningful. Based on each subject's tractogram, we computed individual mean FA connectomes. A node selection for DMN based upon the AAL atlas (Fig. 1) was performed. The nodal degree features for all anatomical nodes in the DMN were extracted and compared across the three groups using one-way ANOVA statistics. The P-values less than 0.05 were considered significant.Results
One-way ANOVA performed showed no significant difference in nodal degree of DMN between the left and right TLE groups. Compared to HC, Right-TLE showed significantly lower local nodal degree in right inferior frontal gyrus orbital part (ORBinf.R), right superior frontal gyrus medial orbital (ORBsupmed.R) and right posterior cingulate gyrus (PCG.R) (Fig.2 A). Compared to HC, Left-TLE cohort showed significantly lower local nodal degree in left hippocampus (HIP.L) and left anterior cingulate and paracingulate gyri (ACG.L) (Fig.2 B).Discussion
According to the structural connectivity, there are significant differences in DMN nodes connectivity among the TLE patients compared to the control cohort. DMN regions with abnormal structural connectivity in TLE subjects corresponded with the epileptogenic brain sides. Based on our results, structural connectivity, as determined by local degree measure, may have a potential application in determining the laterality in cases of TLE.Acknowledgements
We must acknowledge the contribution of the Iranian National Brain Mapping Lab (NBNL) for MRI data acquisition throughout this project. This work was partially funded and supported by Iran’s National Elites Foundation, National Institute for Medical Research Development (Grant No. 971683), and Cognitive Sciences & Technologies Council (Grant No. 6431), between 2017 and 2021.References
1. Engel J. Mesial Temporal Lobe Epilepsy: What Have We Learned? The Neuroscientist. 2001;7(4):340-352. 2. Chiang S, Stern JM, Engel J, Levin HS, et al. Differences in graph theory functional connectivity in left and right temporal lobe epilepsy. Epilepsy Research. 2014;108(10):1770-1781. 3. Tournier, J.-D., Mori, S., Leemans, A., et al. Diffusion tensor imaging and beyond. Magn. Reson. Med.2011; 65: 1532–1556. 4. Smith, R.E., Tournier, J.-D., Calamante, F., Connelly, A., et al. Anatomically-constrained tractography: improved diffusion MRI streamlines tractography through effective use of anatomical information. Neuroimage. 2012; 62: 1924–1938. 5. Smith, R.E., Tournier, J.-D., Calamante, F., Connelly, A., et al. The effects of SIFT on the reproducibility and biological accuracy of the structural connectome. Neuroimage. 2015; 104:253–265.Figures
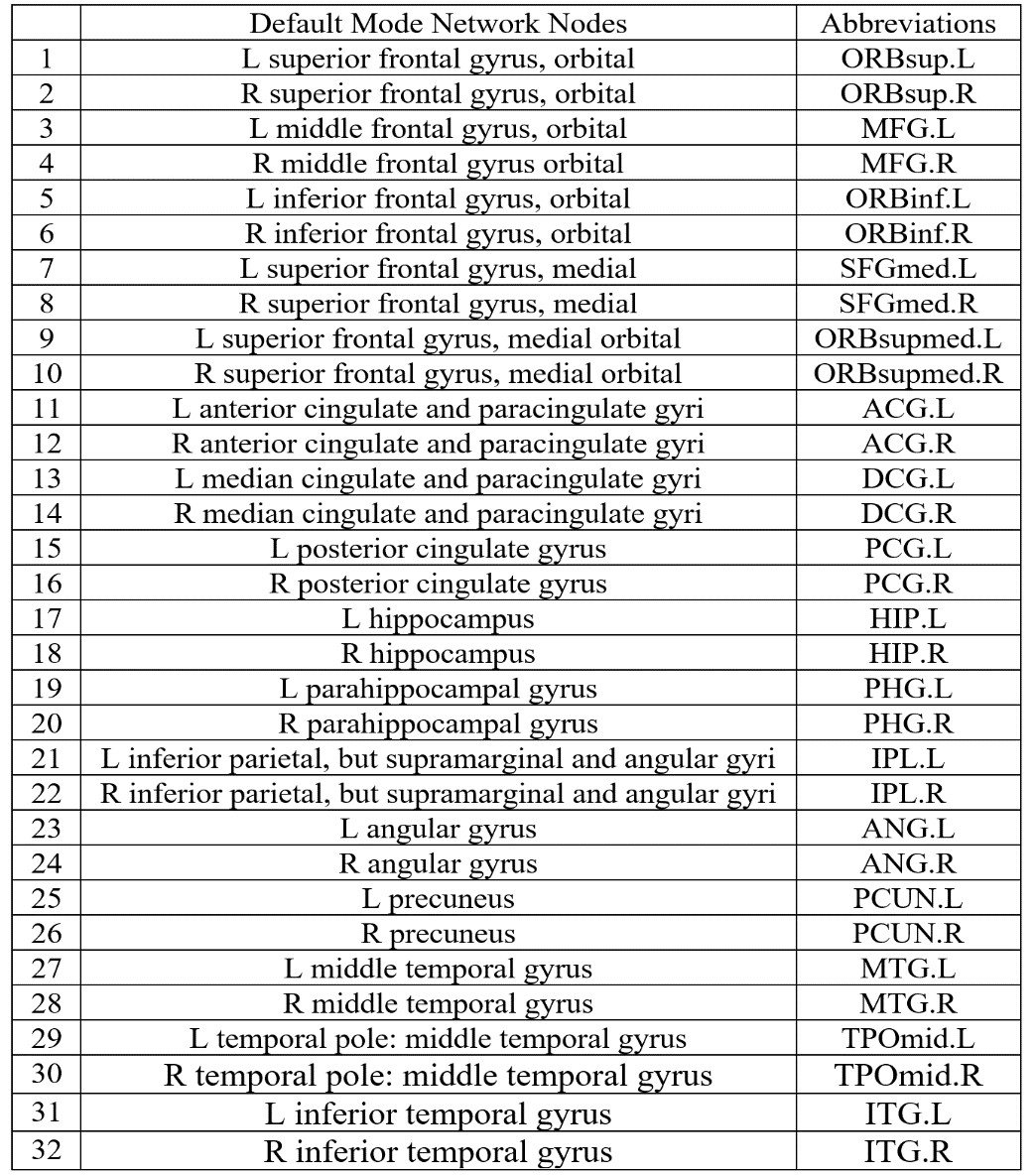
Fig. 1. Default Mode Network Nodes
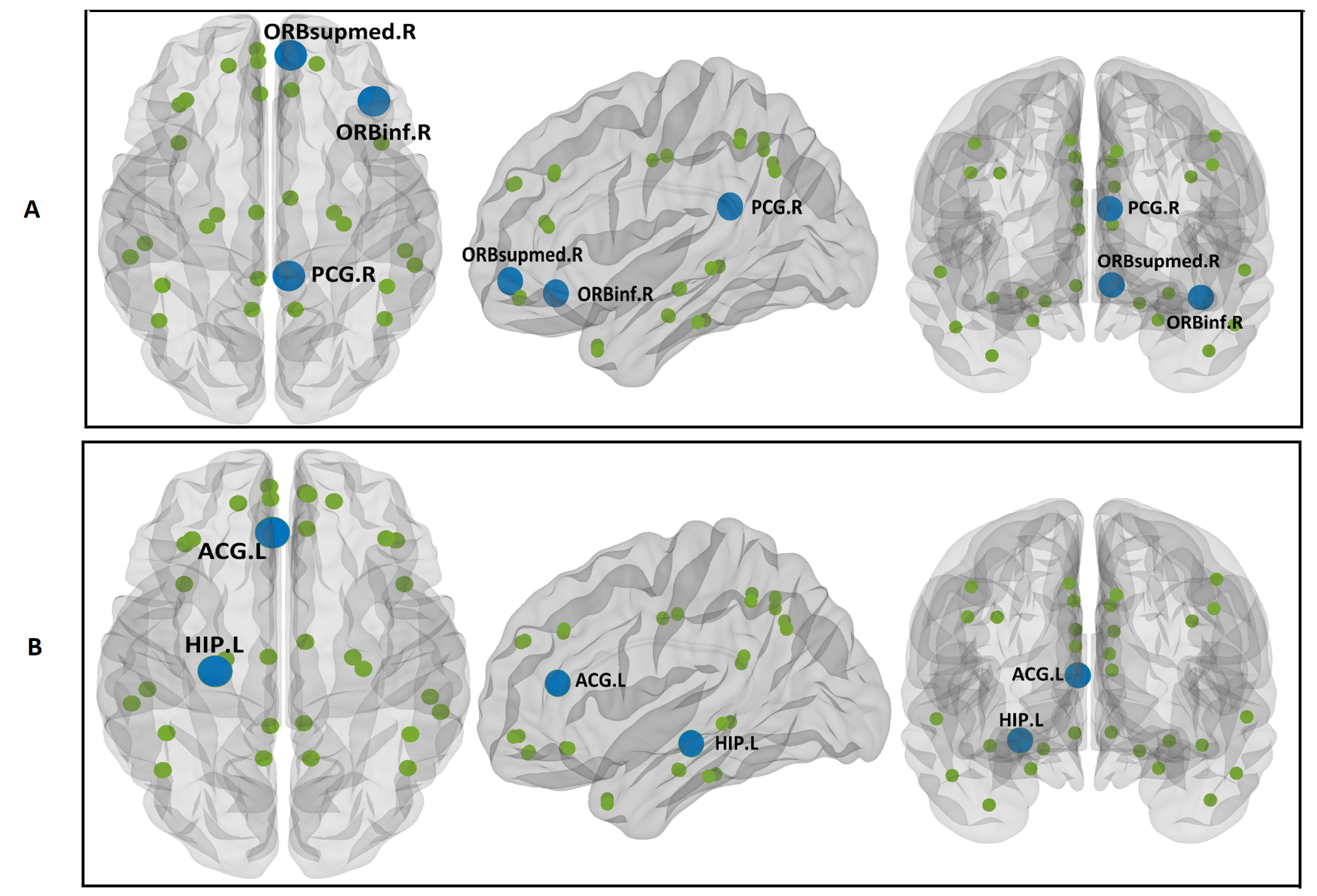
Fig. 2.
A) The First Row: Significant differences in nodal degree in DMN between HC and Right-TLE cohorts
B) The Second Row: Significant differences in nodal degree in DMN between HC and Left-TLE cohorts