1874
Image Quality Transfer improves the potential clinical value of low-field MRI
Matteo Figini1,2, Hongxiang Lin1,2,3, Felice D'Arco4, Godwin Inalegwu Ogbole5, Maria Camilla Rossi Espagnet6, Olalekan Ibukun Oyinloye7, Joseph O Yaria8, Donald Amasike Nzeh7, Mojisola Omolola Atalabi9, Lisa Ronan1,2, David W Carmichael10,11, Judith Helen Cross4,11, Ikeoluwa A Lagunju12, Delmiro Fernandez-Reyes2,12, and Daniel C Alexander1,2
1Centre for Medical Image Computing, University College London, London, United Kingdom, 2Computer Science, University College London, London, United Kingdom, 3Research Center for Healthcare Data Science, Zhejiang Lab, Hangzhou, China, 4Great Ormond Street Hospital for Children, London, United Kingdom, 5Radiology, College of Medicine, University of Ibadan, Ibadan, Nigeria, 6Neuroradiology, Sapienza University, Rome, Italy, 7Radiology, University of Ilorin Teaching Hospital, Ilorin, Nigeria, 8Neurology, University College Hospital Ibadan, Ibadan, Nigeria, 9Radiology, University College Hospital Ibadan, Ibadan, Nigeria, 10School of Biomedical Engineering & Imaging Sciences, King's College London, London, United Kingdom, 11UCL Great Ormond Street Institute of Child Health, London, United Kingdom, 12Paediatrics, College of Medicine, University of Ibadan, Ibadan, Nigeria
1Centre for Medical Image Computing, University College London, London, United Kingdom, 2Computer Science, University College London, London, United Kingdom, 3Research Center for Healthcare Data Science, Zhejiang Lab, Hangzhou, China, 4Great Ormond Street Hospital for Children, London, United Kingdom, 5Radiology, College of Medicine, University of Ibadan, Ibadan, Nigeria, 6Neuroradiology, Sapienza University, Rome, Italy, 7Radiology, University of Ilorin Teaching Hospital, Ilorin, Nigeria, 8Neurology, University College Hospital Ibadan, Ibadan, Nigeria, 9Radiology, University College Hospital Ibadan, Ibadan, Nigeria, 10School of Biomedical Engineering & Imaging Sciences, King's College London, London, United Kingdom, 11UCL Great Ormond Street Institute of Child Health, London, United Kingdom, 12Paediatrics, College of Medicine, University of Ibadan, Ibadan, Nigeria
Synopsis
We applied Image Quality Transfer to enhance the contrast and resolution in the slice direction of low-field structural MRI, using a deep learning model trained on simulated images. Six radiologists blindly reviewed the enhanced images compared to low- and high-field images from 12 paediatric patients with epilepsy. Results demonstrated significant improvement of the visualisation of brain structures in sagittal and coronal orientations, and marginal improvement of the contrast between grey and white matter. If these promising results are confirmed in a larger study and in lesions, IQT could be an important tool to enhance the diagnostic power of low-field MRI.
Introduction
The standard magnetic field for clinical MRI scanners in high-income countries is currently 1.5T or 3T, but low-field (< 1T) scanners are still common in most lower- and middle-income countries, mainly due to infrastructure complexities. In a drive to increase MRI accessibility, interest in open-bore and portable low-field MRI systems has also grown in recent years. Low-field MRI has lower signal-to-noise ratio compared to high-field, and images are usually acquired at lower resolution to partially counteract this loss in signal1. Image Quality Transfer (IQT) is a machine learning framework that aims to estimate, from a low-quality image, the image that would have been obtained from a state-of-the-art scanner on the same subject2-4. We have previously shown IQT enhancement of low-field MRI, quantitatively on simulated images and qualitatively in a few real cases5-7. Here we report the results of a clinical evaluation by 6 radiologists who blindly reviewed and rated the diagnostic quality of low-field, high-field, and IQT-enhanced low-field images from 12 paediatric patients.Methods
Fluid-Attenuated Inversion Recovery (FLAIR), T1-weighted (T1w) and T2-weighted (T2w) images were acquired in axial orientation both on a 0.36T MRI scanner (MagSense 360, Mindray, China) and on a 1.5T scanner (Signa, GE Healthcare, Milwaukee, WI, USA) with an in-plane resolution of 0.5 mm and a slice thickness of 5 mm; 3D T1w images were also acquired at 1.5T as anatomical reference. Twelve paediatric patients with epilepsy were included in this study. Both LF and HF images underwent brain extraction and correction of bias field artifacts; T1w LF images were also corrected for cross-talk artifacts. The IQT model was based on an Anisotropic U-Net5 trained on simulated images; see 7 for details. It was applied to the axial low-field (LF) images to obtain IQT-enhanced images, with improved resolution in the slice direction and 3T-like contrast. The images were anonymized by removing both patient’s data and scanner information, so that readers were blinded to the field strength of the image they were viewing. The images were randomly assigned to 6 reviewers, 2 with specialist expertise for paediatric neuroimages and 4 with general radiology training. A first experiment aimed at evaluating the image resolution in non-axial planes. The two expert reviewers received all the LF, IQT-enhanced and HF images (unlabelled) of 6 patients each; they scored the visualisation of the hippocampus and inferior frontal gyrus on the images reformatted to coronal and sagittal orientation respectively, from 1 (worst) to 4 (best). A second experiment aimed at evaluating in-plane image contrast in the healthy brain. Each reviewer received all the images from 6 patients (a different set than in experiment 1) and was asked to score the contrast between grey and white matter from 1 (not visible) to 4 (very clear).Results
IQT significantly improved the visualization on non-axial planes of the hippocampus and inferior frontal gyrus, as shown by the representative examples of coronal and sagittal reformatted images in Figure 1. Indeed, experiment 1 scores were highest for the IQT-enhanced images, followed by HF and LF (figure 2); the difference between LF and IQT-enhanced scores was significant (Wilcoxon signed-rank test). Figure 3 shows axial images from one representative subject. In experiment 2, the average scores for IQT-enhanced T1w and T2w images were intermediate between LF and HF images (figure 4), and IQT-enhanced T2w images even reached the level of HF. The average scores for IQT-enhanced FLAIR images, on the other hand, were lower than at LF in experiment 2.Discussion and Conclusion
We have shown that our IQT algorithm can improve the spatial resolution of low-field MRI and allows radiologist to visualise brain structures in non-axial orientations when only axial scans with thick slices are acquired, as is often the case in low-field studies when time is limited. We have also shown that it can improve the contrast between brain tissues in T1- and T2-weighted images. However, the FLAIR contrast could not be improved in most cases; this may be due to the fact that IQT relies on the availability of high-quality references for training, which is more limited for FLAIR than it is for T1w or T2w images. If larger collections of high-quality FLAIR images could be used in the future, we expect IQT performance on FLAIR to improve as well. We are currently undergoing a larger study with more subjects, in which the reviewers are evaluating the detectability of epilepsy lesions as well as the image contrast in the healthy brain tissues. If these preliminary results are confirmed, IQT could be an important tool to enhance the diagnostic power of low-field MRI, and have an impact on radiology practice in lower- and middle-income countries, and could be extended to contribute in other clinical imaging scenarios in which high-field MRI is inaccessible for any reason.Acknowledgements
This work was supported by EPSRC grants (EP/R014019/1, EP/R006032/1 and EP/M020533/1) and the NIHR UCLH Biomedical Research Centre.References
- Marques JP, Simonis FFJ, Webb AG. Low-field MRI: An MR physics perspective. Journal of Magnetic Resonance Imaging. 2019; 49(6):1528–1542.
- Alexander DC, Zikic D, Ghosh A, et al. Image quality transfer and applications in diffusion mri. NeuroImage. 2017; 152:283–298.
- Blumberg SB, Tanno R, Kokkinos I, Alexander DC. Deeper image quality transfer: Training low-memory neural networks for 3D images. In International Conference on Medical Image Computing and Computer-Assisted Intervention (MICCAI). 2018: 118–125.
- Tanno R, Worrall DE, Kaden E, et al. Uncertainty modelling in deep learning for safer neuroimage enhancement: Demonstration in diffusion MRI. NeuroImage. 2020; 225:117366.
- Lin H, Figini M, Tanno R, et al. Deep learning for low-field to high-field MR: Image quality transfer with probabilistic decimation simulator. In International Workshop on Machine Learning for Medical Image Reconstruction. 2019: 58-70.
- Figini M, Lin H, Ogbole G, et al. Image Quality Transfer enhances contrast and resolution of low-field brain MRI in african paediatric epilepsy patients. arXiv preprint. 2020: 2003.07216.
- H Lin, Figini M, D’Arco F, et al., Low-to-High Field MR Image Quality Transfer. In Proc. Intl. Soc. Mag. Reson. Med. 2021; 29:3826
Figures
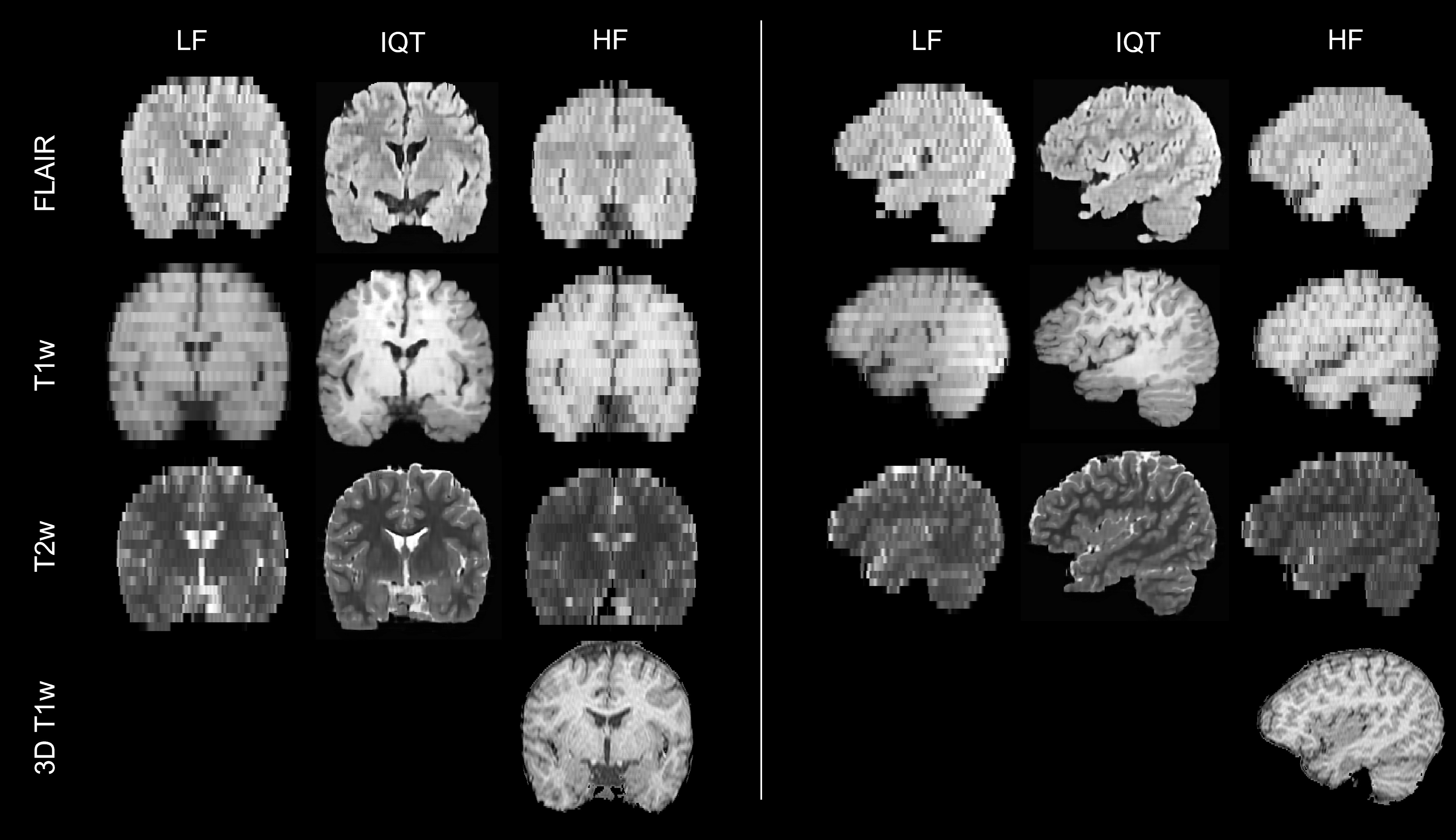
Figure 1: Representative coronal (left) and sagittal (right)
reformatted images from a 13-year-old patient with apparently normal brain MRI.
The 3D T1w image acquired at HF is also reported as reference
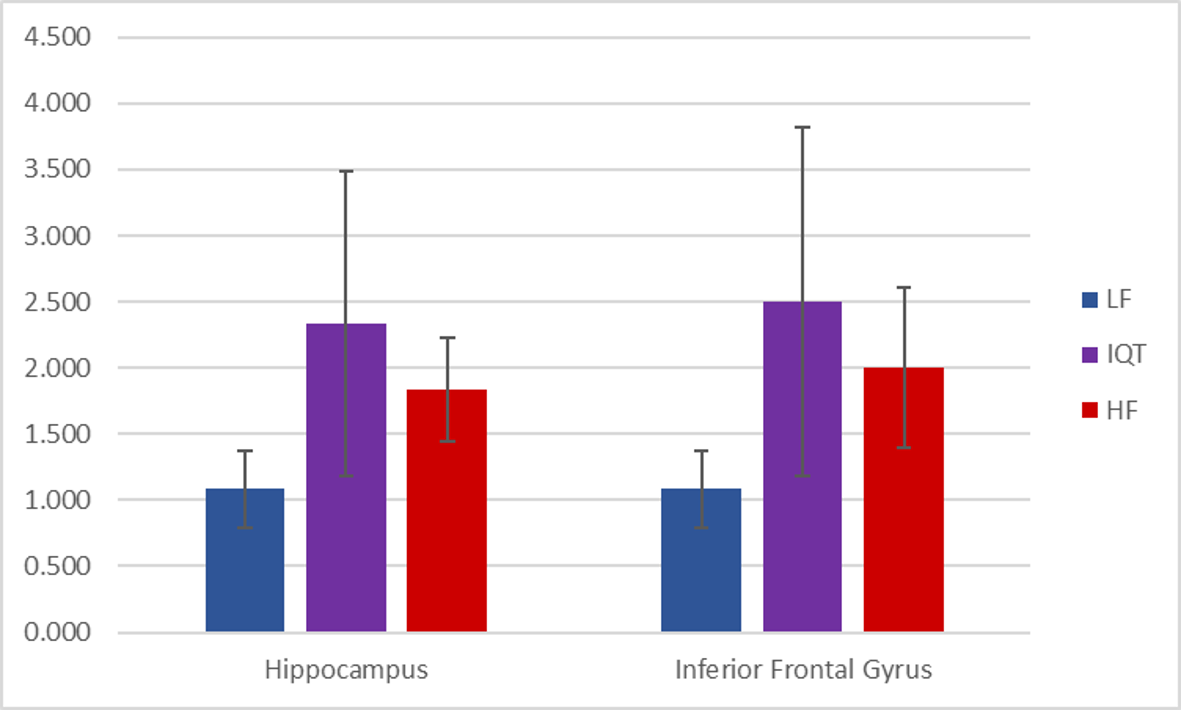
Figure 2: scores for the visualisation of the Hippocampus on
coronal images (left) and of the Inferior Frontal Gyrus on sagittal images (right),
in each group (LF, IQT-enhanced and HF), averaged among the 12 subjects. The
error bars represent standard deviation. The score for each subject accounted for
the visualisation on all of FLAIR, T1w and T2w images.
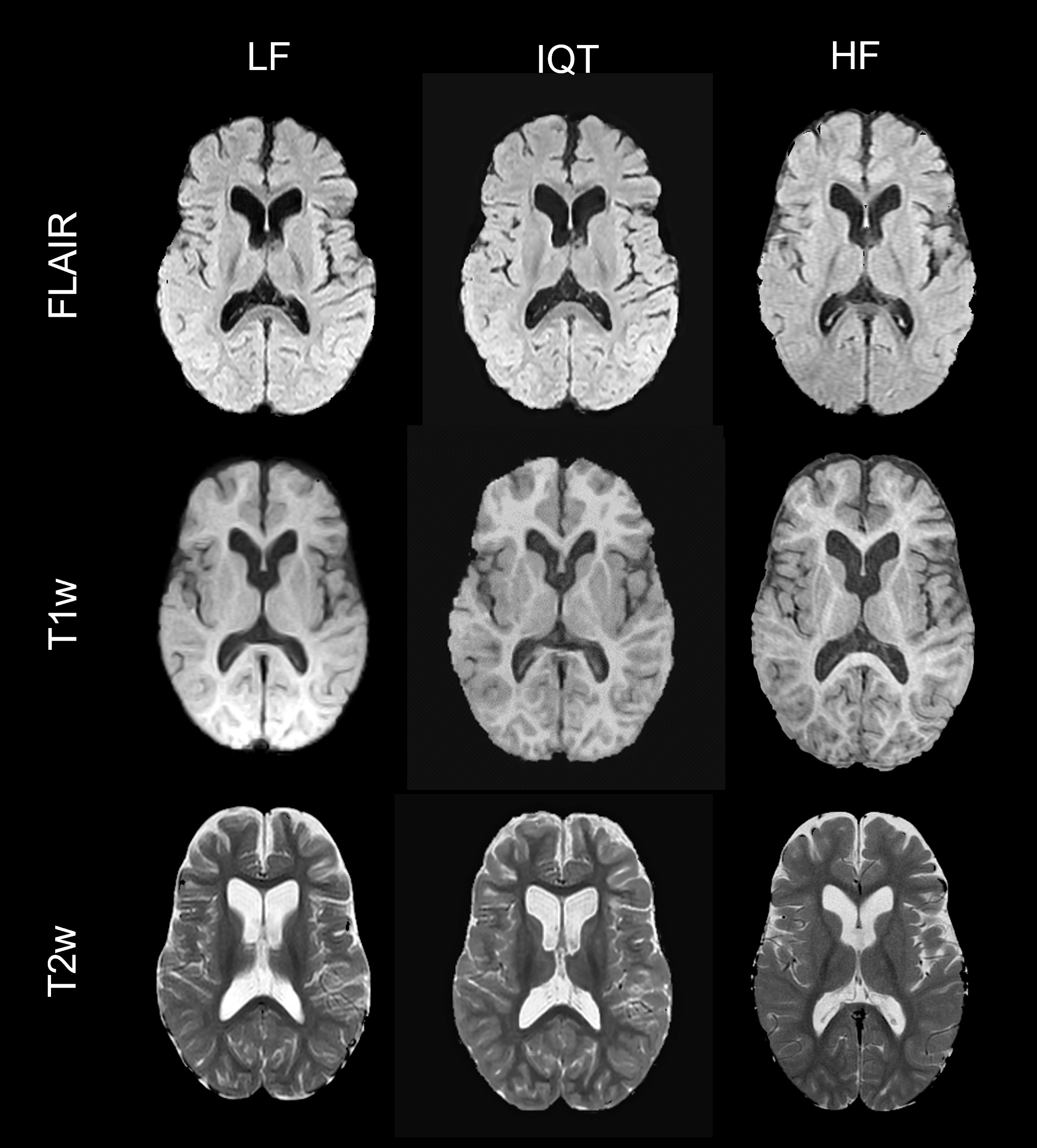
Figure 3: representative LF, IQT-enhanced and HF axial
images for a 5-year-old patient with apparently normal brain MRI
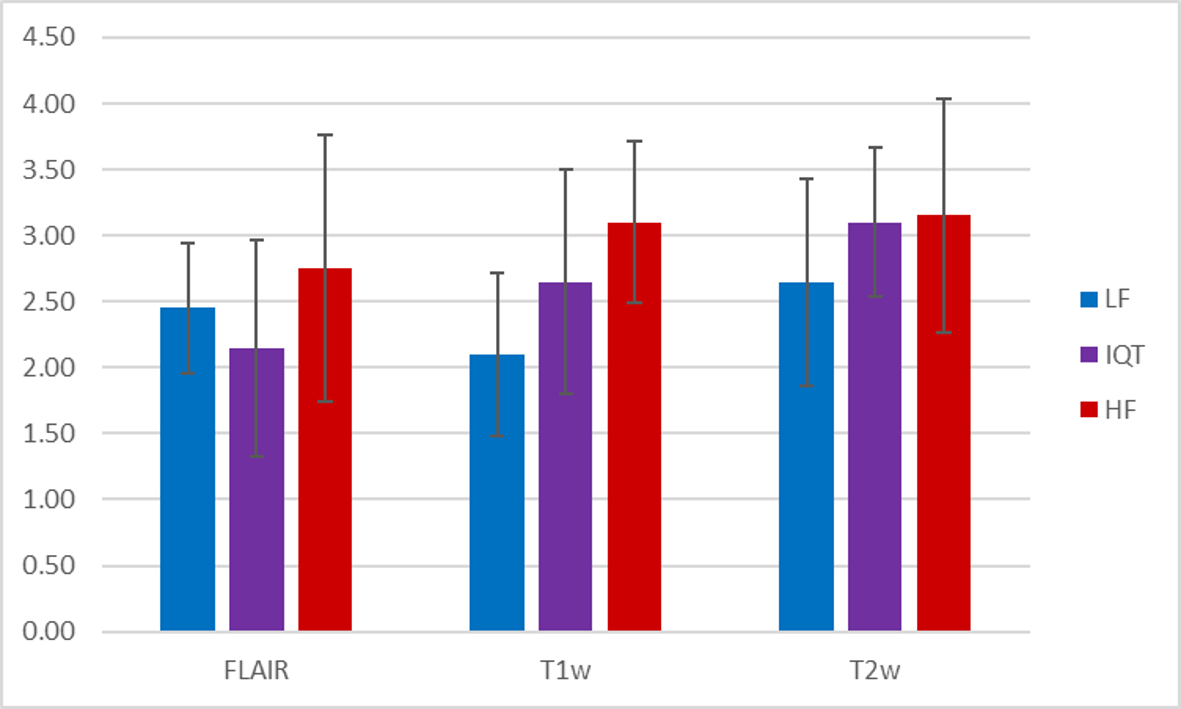
Figure 4: grey/white matter differentiation scores obtained
in experiment 2 by FLAIR (left), T1w (middle) and T2w (right) images in each
group (LF, IQT-enhanced and HF), averaged among the 12 subjects. The error bars
represent standard deviation.
DOI: https://doi.org/10.58530/2022/1874