1847
Biventricular function using a novel real-time free-breathing compressed sensing cine sequence with R-R normalization and motion correction1Radiology, Mayo Clinic, Rochester, MN, United States, 2Siemens Healthineers, Chicago, IL, United States, 3Mayo Clinic, Rochester, MN, United States
Synopsis
CMR is the gold standard for assessing biventricular size and function. bSSFP Seg Cine is a standard cine method, but requires breath-holding which prolongs table time and limits utility in dyspneic patients. A novel real-time technique RTCSCineMoCo combines free-breathing acquisition with compressed sensing and motion correction. In 100 subjects RTCSCineMoCo generated similar results to Seg Cine for LVEF, LV end-diastolic mass, and RVESV with agreement including no difference at Bland-Altman analysis for all LV and RV measures. The shorter table time for RTCSCineMoCo and ability to robustly image dyspneic patients are important enhancements for clinical practice.
Introduction
Cardiac MRI is the reference standard for biventricular size and systolic function. Conventional parallel imaging accelerated segmented balanced steady-state free precession (bSSFP) cine imaging (Seg Cine) is employed in clinical practice, but requires multiple breath-holds to acquire an entire short-axis stack. This prolongs table time and is problematic in dyspneic, sedated, or somnolent patients. Additionally, segmented imaging strategies are limited in patients with arrhythmia even when employing arrhythmia rejection. Novel real-time imaging techniques have been developed to address the breath-holding and scan-time challenges of Seg Cine and thus enhance patient comfort and reduce total table time. However, their clinical application was historically limited due to the lower spatial and temporal resolution compared to Seg Cine. A prototype free-breathing cardiac cine technique with compressed sensing and in-line respiratory motion correction (RTCSCineMoCo) was recently developed and has shown comparable results (both qualitative and quantitative) with the Seg Cine method in a small feasibility study1. The purpose of this study is to compare RTCSCineMoCo performance with the standard-of-reference Seg Cine for assessment of biventricular size and systolic function in a larger cohort of consecutive patients at 1.5T.Methods
Retrospectively, we collected and analyzed data from 107 patients (age ≥ 18 years) who underwent both imaging techniques at a single institution after referral for cardiac MRI. Images were obtained as short-axis (SAX) cine stacks with complete biventricular coverage using a 1.5 T clinical scanner (MAGNETOM Aera, Siemens Healthcare, Erlangen, Germany); RTCSCineMoCo images were pre-contrast, while Seg Cine images were taken after a double dose gadobutrol bolus infusion. Our departmental quality review board approved RTCSCineMoCo usage as an adjunct to the routinely used Seg Cine as an enhancement to the clinical practice. Seg Cine Imaging Parameters: TR/TE 2.87/1.5 ms, FOV 320 mm, temp res 37.3 ms, matrix 224 x 224, slice thickness 6 mm, GRAPPA factor 2, acquisition time / slice 8.5 s / 10 sec pause – 14 HB per slice, acquired at end-inspiration; RTCSCineMoCo parameters: TR/TE 3.07/1.33 ms, FOV 320 mm, temp res 46.05 ms, matrix 192 x 192, slice thickness 8 mm, acquisition time / slice (12 HB / 10.8 sec), acceleration factor 12.8, acquired during free-breathing. Subsequently, biventricular size and systolic function were measured leaving papillary muscles in the blood pool2 using Cvi42 v5.13.5 (Circle Cardiovascular Imaging Inc., Calgary, Canada). The student’s paired t-test (two-sided alpha, p = 0.05) was used to assess statistical significance between quantitative measurements. Bland-Altman plots were generated for the comparisons between techniques. Twenty random subjects were re-analyzed by a single observer to assess for intraobserver variability; Bland-Altman plots were plotted to assess agreement, and Pearson’s correlations were calculated.Results
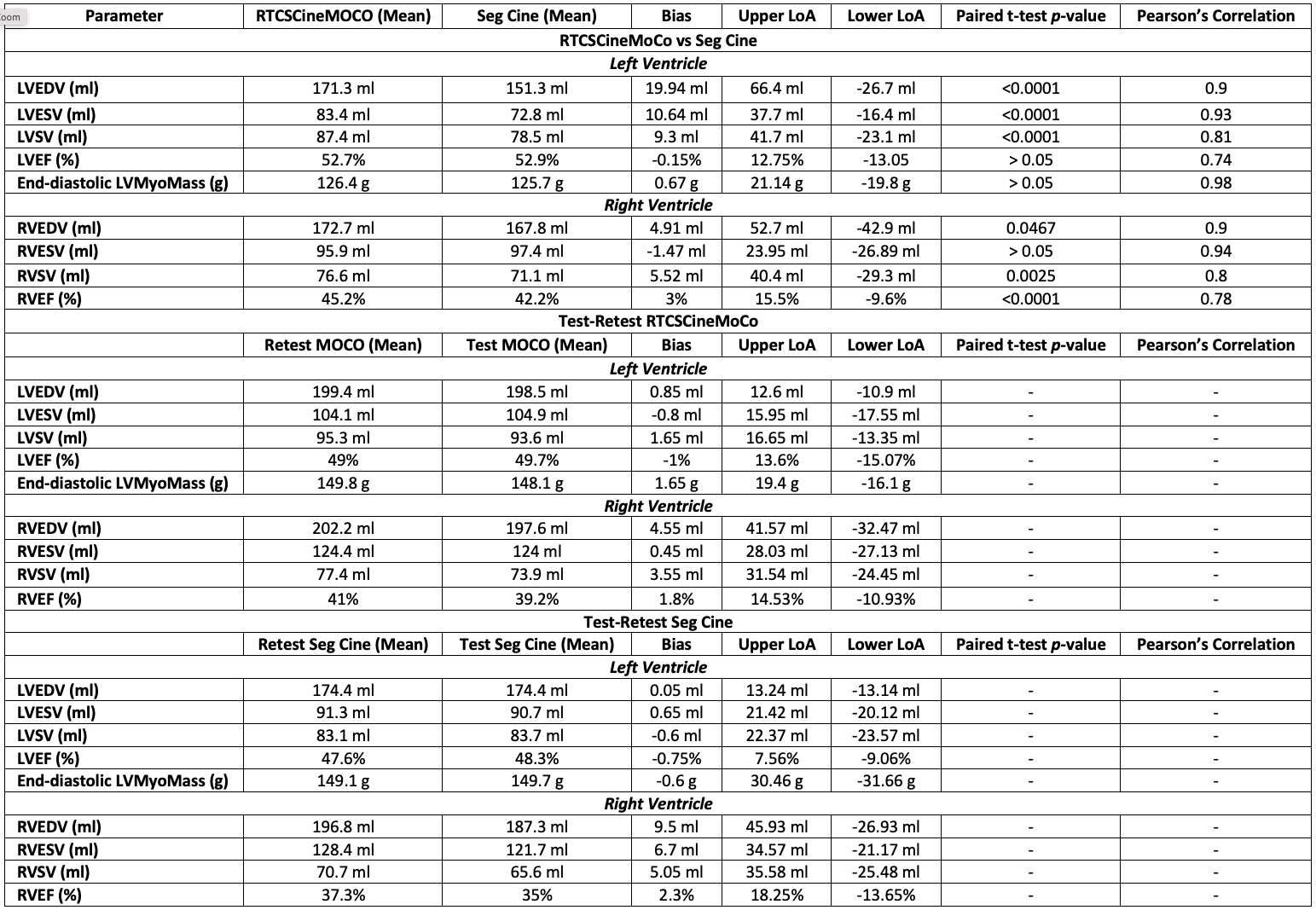
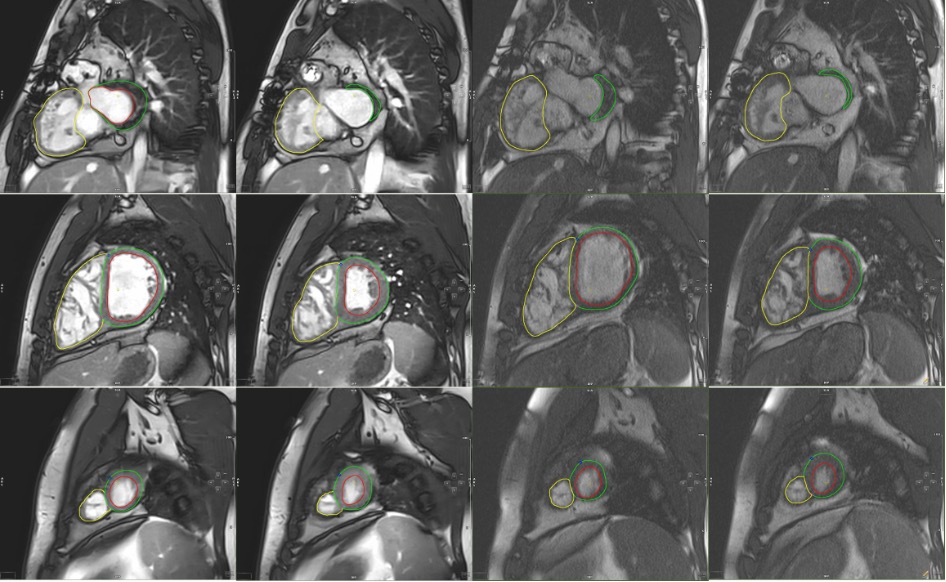
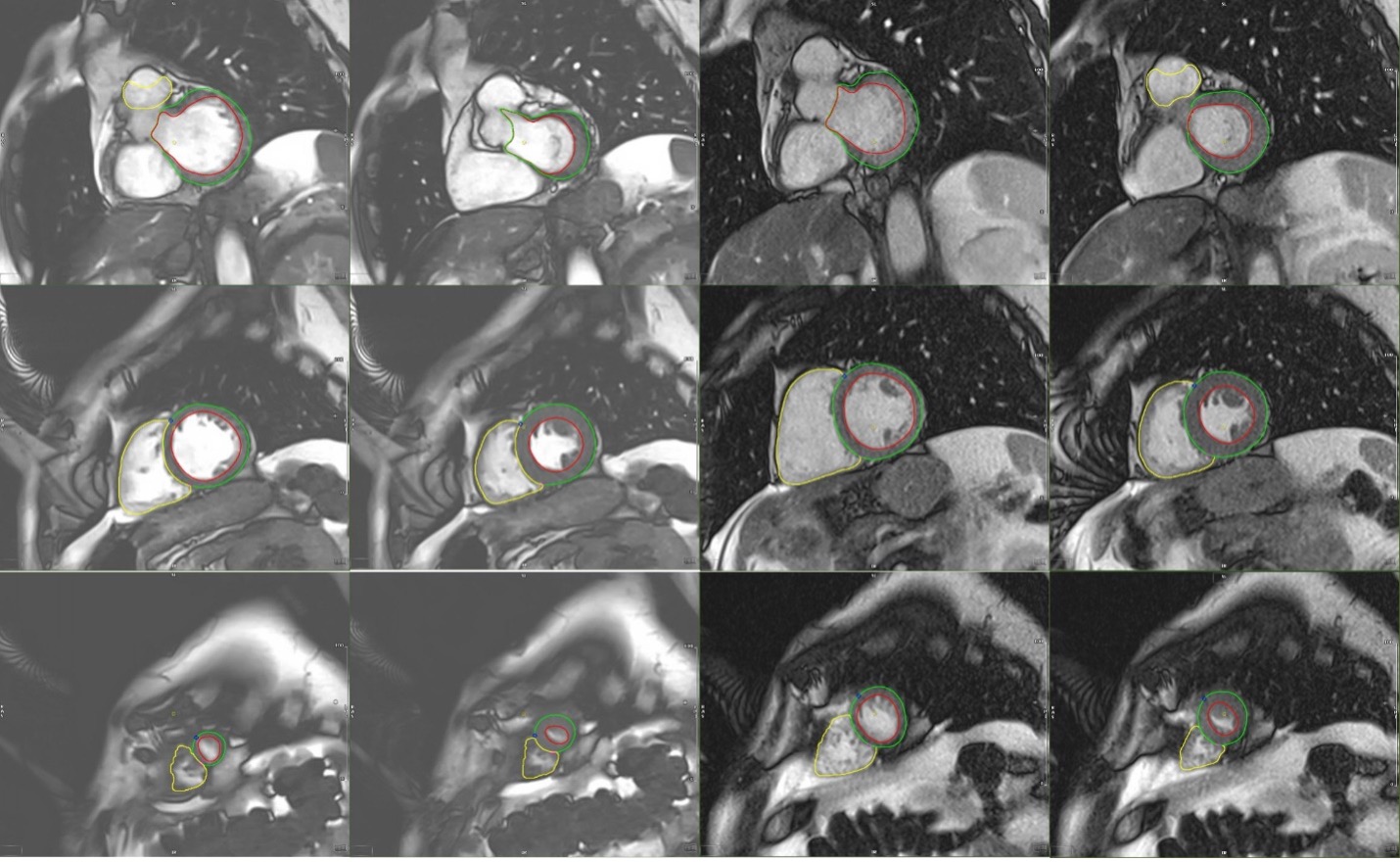
RTCSCineMoCo images were analyzable in all subjects. Seg Cine imaging was limited in 7 patients; these patients were excluded from quantitative analysis. The study sample was therefore comprised of 100 subjects (58 men, average age 57 years). LVEDV, LVESV, LV stroke volume (LVSV), RVEDV, RVSV, and RVEF were statistically significant between techniques with positive bias at Bland-Altman analysis; means of RVESV, LVEF and LV end-diastolic myocardial mass were similar (Figure 1). Representative images from two patients are provided in Figures 2 and 3. Test-retest analysis showed good within method reproducibility at Bland Altman analysis.Conclusion
RTCSCineMoCo images were analyzable in all subjects and compared favorably with conventional Seg Cine, with similar measures of RVESV, LVEF and LV end-diastolic myocardial mass. Although there were differences in other parameters between methods, the magnitude of the bias was small and the confidence interval included no difference. These differences could be related to respiratory phase (breath-holding versus free-breathing) or blood pool – myocardial conspicuity between non-contrast and contrast-enhanced cine imaging. RTCSCineMoCo has the potential to shorten table time and improve patient tolerance for cardiac MR allowing time for additional imaging techniques and reserving breath-hold capacity for other essential protocol components.Acknowledgements
No acknowledgement found.References
1. Pang, J. et al. Free-Breathing Cardiac Cine MRI with Compressed Sensing Real-Time Imaging and Retrospective Motion Correction. Proceedings of ISMRM 2020, p 2190.2. Leiner, T. et al. SCMR Position Paper ( 2020 ) on clinical indications for cardiovascular magnetic resonance. Journal of Cardiovascular Magnetic Resonance (BioMed Central, 2020). doi:10.1186/s12968-020-00682-4.
Figures