1843
Real-time Cardiac MRI at 0.55T using through-time spiral GRAPPA
Alexander Fyrdahl1 and Nicole Seiberlich1
1Radiology, University of Michigan, Ann Arbor, MI, United States
1Radiology, University of Michigan, Ann Arbor, MI, United States
Synopsis
Through-time non-Cartesian GRAPPA can be used to enable real-time imaging for evaluation of left-ventricular function. However, it requires arrays with many receiver coils for the parallel imaging reconstruction and gradient systems capable of playing out the specified non-Cartesian trajectories. In this work, we explore the use of non-Cartesian GRAPPA for real-time cardiac imaging on a 0.55T system with lower performance gradients, reduced receiver coils compared to conventional MRI systems.
Introduction
The purpose of this abstract is to demonstrate the feasibility of real-time cardiac imaging on a commercial low field MRI system, without access to cardiac-optimized receiver coils, ECG-gating or high-performance gradients otherwise found in commercial MRI systems. Cine imaging, used to assess cardiac function and wall motion, is an essential component of cardiac MRI. Most cine images are collected using segmented ECG-gated acquisitions, where different portions of k-space are collected over multiple heartbeats, resulting in cardiac images with a high spatiotemporal resolution. Cine imaging is commonly performed at 1.5T, but can also be performed at lower field strengths (1) given appropriate hardware with sufficient receiver coils and gradients, and the ability to gate. However, low-cost, low-field systems designed for use in lower-resource areas may not be equipped with the gating hardware or software required for cine imaging, nor may dedicated CMR-trained operators be on-hand for complex gated acquisitions. Real-time imaging may be more suitable for such scenarios, where no gating is required, simplifying the collection of such images. Non-Cartesian GRAPPA has been shown to enable real-time cardiac imaging, but requires arrays with many receiver coils for parallel imaging reconstruction and gradient systems capable of playing out specified non-Cartesian trajectories. This work explores the use of non-Cartesian GRAPPA for real-time cardiac imaging on a 0.55T system with lower performance gradients, reduced receiver coils compared to conventional MRI systems, and no ability to gate.Methods
Data were acquired in two healthy volunteers at 0.55T (MAGNETOM Free.Max, Siemens Healthcare, Erlangen, Germany) using a prototype spiral bSSFP sequence with a time-optimized M1-compensated variable density spiral trajectory (2) requiring 48 arms to fully sample the edge of k-space. The relevant sequence parameters were: FOV = 300x300 mm, in-plane resolution = 2.34x2.34 mm2, slice thickness = 8 mm, 9–10 slices, TE/TR = 1.4/7.2 ms, flip angle = 68–70 degrees. The maximum gradient amplitude of the low-field system was Gmax = 25 mT/m and the maximum slew rate was Smax = 40 mT/m/ms. Only 15 receiver coil elements were available; 6 anterior surface coil elements and 9 posterior spine coil elements. Fully-sampled data (48 spiral arms) were acquired for GRAPPA calibration, along with accelerated scans (R = 4 and R = 6) corresponding to temporal resolutions of 86.4 ms (11.6 frames/second) and 57.6 ms (17.4 frames/second). A schematic overview of the sampling pattern can be seen in Figure 1. Data were collected during free-breathing, and no gating hardware was applied. The images were reconstructed in MATLAB (MathWorks, Natick, MA) using a previously described through-time GRAPPA reconstruction (3). For comparison, the same volunteers were scanned in a 1.5T MRI system (MAGNETOM Sola, Siemens Healthcare, Erlangen, Germany) with an ECG-gated Cartesian cine acquisition (25 cardiac phases), and a breathhold Cartesian real-time acquisition with a temporal resolution of 43.6 ms (22.9 frames/second). All images were imported into Segment 3.2 R8757 (Medviso, Lund, Sweden) for analysis (4). Left-ventricular segmentation was performed semi-automatically with the built-in AI-segmentation tool, and the endocardial contour was manually adjusted if necessary.Results
In-vivo images from the two volunteers are presented in Figure 2. As the real-time imaging was performed under free-breathing, the real-time image frames were manually matched to the breath-held and triggered images. For volunteer 1, the ejection fraction was measured to 64% for the gold-standard cine, 62% for Cartesian realtime, 62% for spiral realtime with R = 4, and 64% for spiral realtime with R = 6. For volunteer 2, the corresponding measured EF values were 58% for the gold-standard cine, 56% for Cartesian real-time imaging, 55% for spiral real-time imaging with R = 4, and 56% for spiral real-time imaging with R = 6.Discussion
The limited gradient performance requires special consideration when designing spiral trajectories, and the limited number of receiver channels is a challenge for highly accelerated parallel imaging. However, these results suggest that real-time imaging with through-time GRAPPA is feasible at 0.55T with lower performance hardware and no ability to gate. Left ventricular segmentation was performed and agreement was found between the gold-standard cine and the real-time techniques, corroborating previous findings that ejection fraction can be reliably measured from free-breathing real-time images (4).Conclusion
We have demonstrated that, even with the limited gradient performance and sub-optimal coils, through-time spiral GRAPPA is feasible at 0.55T, and provides real-time cardiac image quality that is comparable to cardiac images collected at higher field strengths.Acknowledgements
No acknowledgement found.References
1. Bandettini WP, Shanbhag SM, Mancini C, et al. A comparison of cine CMR imaging at 0.55 T and 1.5 T. J. Cardiovasc. Magn. Reson. 2020;22:1–10.2. Hargreaves BA, Nishimura DG, Conolly SM. Time-Optimal Multidimensional Gradient Waveform Design for Rapid Imaging. Magn. Reson. Med. 2004;51:81–92.
3. Seiberlich N, Lee G, Ehses P, Duerk JL, Gilkeson R, Griswold M. Improved temporal resolution in cardiac imaging using through-time spiral GRAPPA. Magn. Reson. Med. 2011;66:1682–1688.
4. Heiberg E, Carlsson M, Arheden H, Ugander M, Sjögren J, Engblom H. Design and validation of Segment - freely available software for cardiovascular image analysis. BMC Med. Imaging 2010;10:1–13.
5. Aandal G, Nadig V, Yeh V, Rajiah P, Jenkins T, Sattar A, Griswold M, Gulani V, Gilkeson RC, Seiberlich N. Evaluation of left ventricular ejection fraction using through-time radial GRAPPA. J. Cardiovasc. Magn. Reson. 2014;16:1–13.
Figures
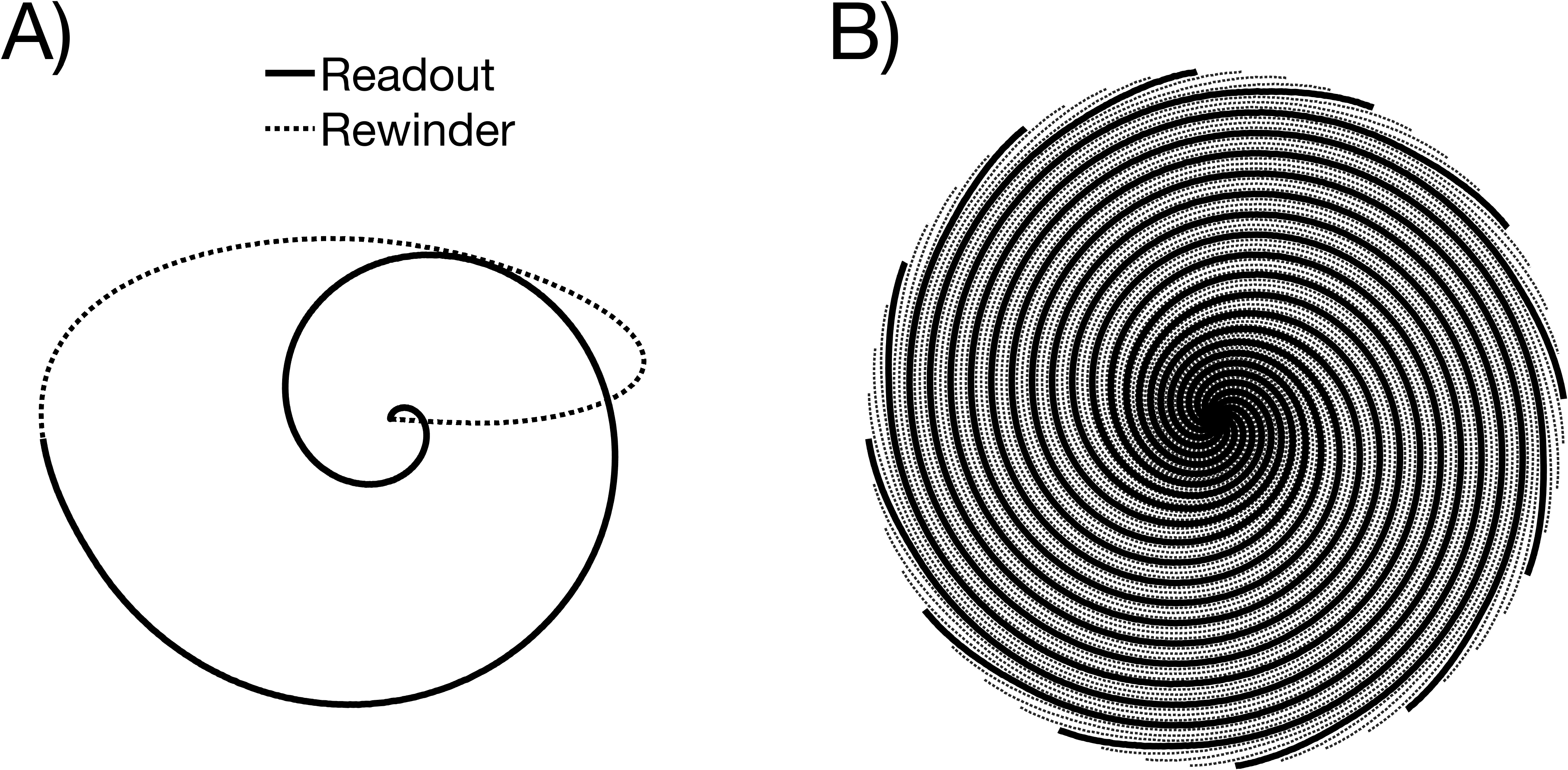
Figure 1. A) One interleaf of the spiral trajectory designed for low-field real-time imaging. The solid line represents the readout portion, whereas the dotted line represents the time-optimized M0 and M1-compensated rewinding portion. B) The full sampling pattern, where the solid lines represent the spiral arms acquired with an acceleration factor of R = 4 and the solid and dotted lines together represents the fully sampled acquisition used for GRAPPA calibration.
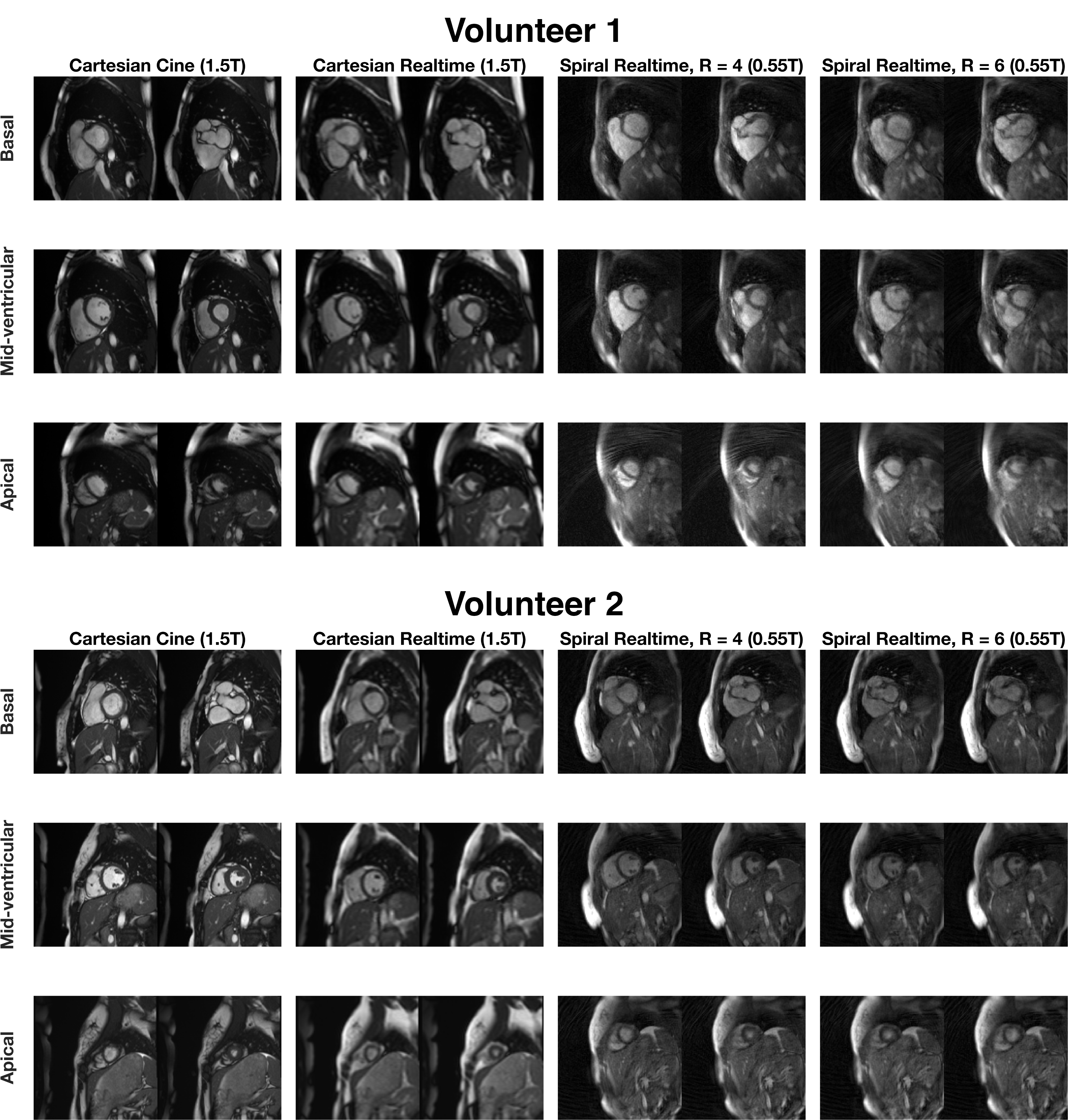
Figure 2. Short axis stacks from both volunteers showing gold standard ECG-gated Cartesian cine images (1.5T), Cartesian real-time images (1.5T) and spiral real-time images (R = 4 and R = 6) collected at 0.55T. The respiratory position of the free-breathing spiral images has been manually matched to the breath-held and triggered images.
DOI: https://doi.org/10.58530/2022/1843