1809
Ultra-Fast Water/Fat Imaging of the Abdomen at 0.55T1Ming Hsieh Department of Electrical and Computer Engineering, University of Southern California, Los Angeles, CA, United States, 2Department of Biomedical Engineering, University of Southern California, Los Angeles, CA, United States, 3Siemens Medical Solutions USA, Inc., Los Angeles, CA, United States
Synopsis
We demonstrate single-breath-hold volumetric water/fat imaging of the abdomen using spiral gradient echo imaging at 0.55T. This provides 4x finer spatial resolution with adequate SNR and spatial resolution to measure the visceral adipose tissue compartment.
Introduction
Non-invasive body composition assessment is an essential part of our arsenal for monitoring obesity and evaluating the effectiveness of interventions (e.g., diet, exercise, surgery). High end modalities like CT and MRI are used extensively for evaluating the spatial distribution of adipose tissue, including visceral and subcutaneous compartments. MRI is also the non-invasive gold standard for evaluating intramuscular fat and liver fat. These technologies have made it possible to evaluate dietary and exercise interventions on a short timescale.In this work, we investigate opportunities for improved body composition imaging at the lower MRI field strength of 0.55 Tesla (1). These systems provide reduced susceptibility effects, improved imaging around air-tissue interfaces, and metallic implants, and new flexibility in the MRI pulse sequences. These systems are well-suited for body imaging, demonstrating liver iron overload assessment (2) and diagnostic abdominal imaging (3).
This work is particularly inspired by recent work by Guenthner et al. using spiral multiecho imaging at 0.75T (4). Here, we demonstrate volumetric single breath hold F/W imaging covering the entire visceral cavity, with high spatial resolution, and no major artifacts around the gastrointestinal tract.
Methods
Experimental Methods: Experiments were performed using a whole body 0.55T system (prototype MAGNETOM Aera, Siemens Healthineers, Erlangen, Germany) equipped with high-performance shielded gradients (45 mT/m amplitude, 200 T/m/s slew rate). Data collection used a 6-channel body array (anterior) and 6 elements from a table-integrated 18-channel spine array (posterior). Four healthy volunteers (2M/2F, Age 22-45) were scanned under a protocol approved by our Institutional Review Board, after providing written informed consent.Imaging Parameters: All scans were multi-echo gradient-recalled echo (GRE) and contained a single 208 mm 3D slab of the abdomen from top of liver to pelvis. Cartesian 3D GRE with volumetric interpolated breath-hold examination (VIBE) and prototype stack-of-spiral sequences (5) were designed to utilize the same breath-hold duration (16-sec for 2 echo, and 22-sec for 3-echo). Table 1 summarizes the scan parameters.
Reconstruction and Analysis: All individual echoes were reconstructed online using CAIPIRINHA (6) for cartesian and SPIRIT (7) for spiral acquisitions. Water/Fat separation was performed using the region-growing IDEAL approach (8), as implemented in the open-source 2012 ISMRM Water/Fat Reconstruction Toolbox (9).
Results
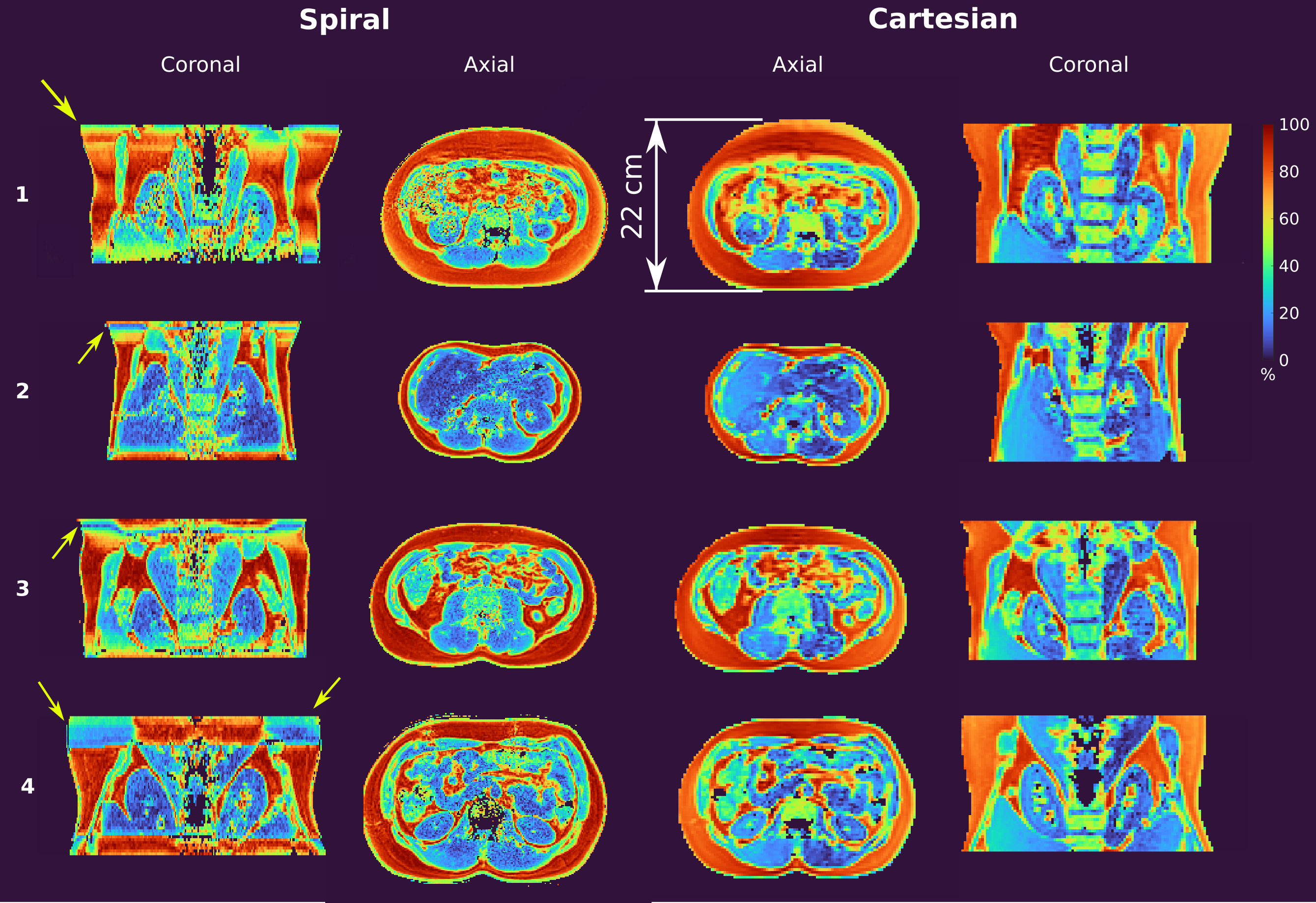
Figure 2 contains panning axial movies from one representative subject. Shown are the individual echo images, and the reconstructed W, F, ∆f, and PDFF images, for Cartesian and Spiral 3-echo imaging. The SNR is adequate, and W-F separation is effective. PDFF maps show reasonable values (92±3%) in subcutaneous and visceral adipose tissue (SAT and VAT).Figure 3 contains multi-planar reformats from the Cartesian and Spiral 3-echo datasets from all four subjects. The spiral approach provides superior spatial resolution in the same scan time, which is particularly noticeable in the visceral cavity (e.g., definition of visceral organs and visceral adipose tissue). The spiral approach suffers from F/W separation errors in slices further from isocenter in the S/I direction (arrows), which we suspect is due to shimming and concomitant field effects.
Discussion
Multi-echo Spiral-based F/W imaging at 0.55 Tesla works well and provides a substantial improvement in efficiency over standard Cartesian approaches. This directly translates to 2x finer spatial resolution for single breath-hold whole-abdomen imaging. We were surprised to find that 2mm isotropic resolution in a single breath-hold provided adequate SNR, image quality, and PDFF maps.At conventional field strengths (1.5T and 3T) similar spiral-based approaches have required joint reconstruction (with integrated deblurring) and water/fat separation (10). This approach will be beneficial at lower field strengths, especially when using longer readouts >6 msec (4). In this work, we used very short readouts (3 msec), resulting in minimal blurring when performing reconstruction and F/W separation in two sequential steps. This is because the FW shift is ~80Hz at 0.55T, resulting in negligible point-spread-function distortion.
Future work includes exploring longer readouts for even greater scan efficiency, GIRF-based trajectory correction, integrated concomitant field and gradient nonlinearity correction, and application to challenging scenarios such as pediatric obesity imaging.
Conclusion
Single-breath-hold volumetric water/fat imaging of the human abdomen is feasible at 0.55T and provides adequate SNR and spatial resolution to measure the VAT compartment.Acknowledgements
We acknowledge grant support from the National Science Foundation (#1828736) and research support from Siemens Healthineers.References
1. Campbell-Washburn AE, Ramasawmy R, Restivo MC, Bhattacharya I, Basar B, Herzka DA, et al. Opportunities in interventional and diagnostic imaging by using high-performance low-field-strength MRI. Radiology. 2019;293(2):384–93.
2. Campbell-Washburn AE, Mancini C, Conrey A, Edwards L, Shanbhag S, Wood J, et al. Evaluation of Hepatic Iron Overload Using a Contemporary 0.55 T MRI System. J Magn Reson Imaging. 2021;
3. Chandarana H, Bagga B, Huang C, Dane B, Petrocelli R, Bruno M, et al. Diagnostic abdominal MR imaging on a prototype low-field 0.55 T scanner operating at two different gradient strengths. Abdom Radiol. 2021;
4. Guenthner C, Dillinger H, Boernert P, Kozerke S. Three-Point Abdominal Water/Fat Separation using a Lower-Field 0.75T MRI. In: Proc ISMRM 2021. 2021. p. 3844.
5. Mugler JP, Fielden SW, Meyer CH, Altes TA, Miller GW, Stemmer A, et al. Breath-hold UTE Lung Imaging using a Stack-of-Spirals Acquisition. In: Proc ISMRM. 2015. p. 1476.
6. Breuer F a, Blaimer M, Mueller MF, Seiberlich N, Heidemann RM, Griswold M a, et al. Controlled aliasing in volumetric parallel imaging (2D CAIPIRINHA). Magn Reson Med. 2006 Mar;55(3):549–56.
7. Lustig M, Pauly J. SPIRiT: Iterative self-consistent parallel imaging reconstruction from arbitrary k-space. Magn Reson Med. 2010 Aug 1;64(2):457–71.
8. Yu H, McKenzie CA, Shimakawa A, Vu AT, Brau ACS, Beatty PJ, et al. Multiecho reconstruction for simultaneous water-fat decomposition and T2* estimation. J Magn Reson Imaging. 2007;26(4):1153–61.
9. Hu HH, Börnert P, Hernando D, Kellman P, Ma J, Reeder S, et al. ISMRM workshop on fat-water separation: Insights, applications and progress in MRI. Magn Reson Med. 2012 Aug 1;68(2):378–88.
10. Brodsky E, Holmes J, Yu H, Reeder S. Generalized k-space decomposition with chemical shift correction for non-Cartesian water-fat imaging. Magn Reson Med. 2008 May 1;59(5):1151–64.
Figures

Table 1: Scan Parameters for Cartesian and Spiral multi-echo GRE at 0.55 Tesla. Common parameters were: Single breath hold; 1 NEX; 15.7° flip angle; 208 mm FOV in the S/I direction with 52 slices each 4 mm thick; 38.5% slice oversampling; 450 mm in-plane FOV. Receiver Coil: Spine 18 + Body 6.