1779
Attenuation Correction in PET/MRI Pediatric Treated Brain Tumors: a Preliminary Comparison between the ZTE and Atlas Techniques1Nuclear Medicine, IRCCS San Raffaele Scientific Institute, Milan, Italy, 2Neuroradiology Unit, IRCCS San Raffaele Scientific Institute, Milan, Italy, 3Department of Medical Oncology and Hematology, Pediatric Oncology Unit, Fondazione IRCCS Istituto Nazionale dei Tumori, Milan, Italy, 4Unit of Bioinformatics and Biostatistics, Department of Applied Research and Technological Development, Fondazione IRCCS Istituto Nazionale dei Tumori, Milan, Italy, 5Vita-Salute San Raffaele University, Milan, Italy
Synopsis
A preliminary comparison between the two Atlas and ZTE attenuation correction methodologies in a group of pediatric patients with brain tumors is presented. The differences of the two ACmaps and PET images were calculated and the PET parameters were compared. Our results show that using ZTE or Atlas to generate ACmaps modifies the SUVs, but the differences in values are very small. Moreover, when metallic artefacts occur, both ZTE and Atlas show loss of signals but ACmapsAtlas has smaller artefacts.
INTRODUCTION
Magnetic Resonance Imaging (MRI) plays a key role in pediatric brain tumors, for diagnosis, response assessment and follow-up monitoring. Nevertheless, differentiating tumor recurrence from pseudo-progression or other treatment-induced reactions after radiation therapy and chemotherapy is challenging on conventional diagnostics, but clinically relevant. Positron Emission Tomography (PET) imaging with 11C-Methionine would improve diagnostic accuracy for the detection of recurrent tumor as compared with MRI alone1. The use of simultaneous hybrid PET/MRI is highly beneficial in children as it allows for a one-stop-shop examination that limits the scanning procedures, the need for a second sedation and also reduces the radiation dose compared to PET/CT. One of the major challenges for PET/MRI is the attenuation correction that, in brain, is performed with Atlas2, with Zero Echo Time/Ultrashort Echo Time (ZTE/UTE) sequences3 or, more recently, with Deep Learning-based methods4. In pediatric patients, and in particular in oncological pediatric studies where tumor resection may occur, the size and the abnormal shape of the head maybe critical for a good attenuation correction. In this work, we have compared the two Atlas and ZTE attenuation correction methodologies in a group of treated pediatric patients with brain tumors. As we do not have gold standards (CT-based ACmaps) for ethic reasons, we have calculated the differences of the two ACmaps and PET images and compared the PET parameters.SUBJECTS AND METHODS
Nineteen children and adolescents (age 10.1±4.5 years, min/max = 2.6/17.7 years, 8/11F/M) with treated high grade brain tumors (five high grade gliomas, six medulloblastomas, four germinomas, one pinealoblastomas, three ependymomas) were scanned on the SIGNA PET/MR scanner (GE Healthcare, Waukesha, WI, USA) using a 32-channel brain coil as part of an approved research protocol for the suspicious of tumor recurrence. Six of them were sedated. The patients were injected with a dose of 11C-Methionine per 1.7 m2of body surface area. The following optimized protocol was used: first, some of the diagnostic MR sequences were acquired soon after the injection of Methionine, then, the simultaneous PET/MRI acquisition started after 25 minutes to wait for the distribution of the tracer in the brain. The PET scan lasted 20 minutes during which we acquired: first, a two-point Dixon (LAVA-flex) and a ZTE sequence with 2.4mm isotropic resolution for generation of the ACmaps, then the clinical coronal T2, 3D Flair, axial T1 pre-contrast, axial DWI sequences. After PET, we completed the examination with the perfusion and post contrast MR sequences. PETZTE and PETAtlas images were retrospectively reconstructed with the TOF-OSEM (3 algorithm iterations, 16 subsets, with PSF modelling, attenuation, scatter correction) using the two ACmaps. The maximum and mean value SUVs on the 42% isocontour VOIs (SUVmax and SUVmean, respectively) were calculated for the lesions on both reconstructed PET images by an expert nuclear medicine physician using the AW server Workstation (GE Healthcare, Waukesha, WI, USA) and compared. Dice index between VOIs has been calculated.RESULTS
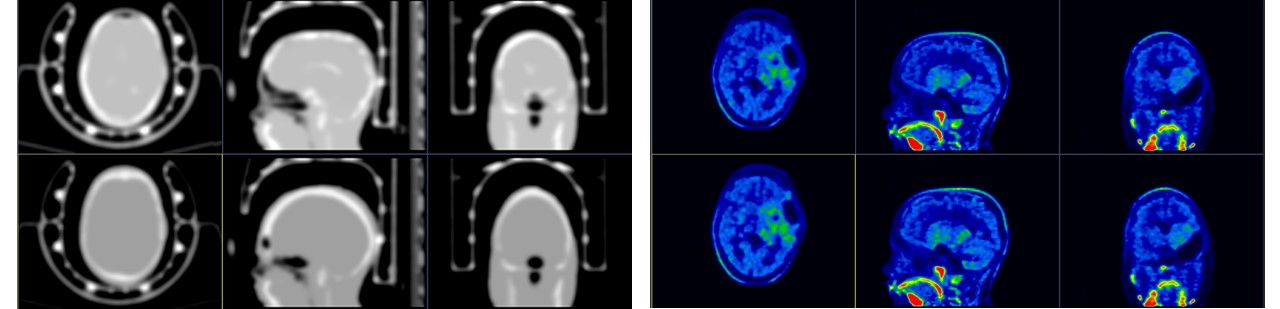
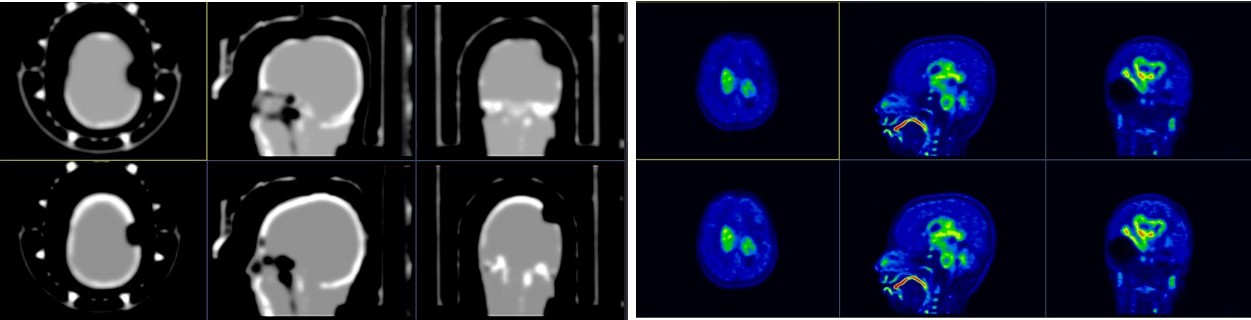
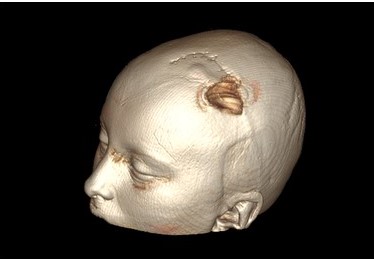
Eight/19 patients had a positive uptake in PET images. Two patients showed artifacts on the MR images due external ventricular drain catheter valve (EVC). Figure 1 shows an example of ACmapZTE and ACmapAtlas and the corresponding PET images for a subject 10 years old. Figure 2 shows an example of ACmaps from ZTE and Atlas and the corresponding PET images for a subject 11 years old with an EVC valve. In Figure 3 the volume rendering of the 3D FSPGR sequence of the same patient of Figure 2 is shown. In Figure 4 the table with SUVmean, SUVmax and Volumes of each patients. The SUV values calculated using ACmapAtlas are always higher than the ones calculated using ACmapZTE. The corresponding volumes of the VOIs are variable. The mean values of the difference % between SUVmax is -0,103, SUVmean is -0,060 and Volume is -0,016. The Dice mean value is 0.98952.DISCUSSION AND CONCLUSIONS
This preliminary work on the effect of attenuation correction on PET images of brain tumor pediatric patients shows that using of ZTE or Atlas for the generation of ACmaps can modify the SUVs of the study but the differences in the values are very small. The corresponding DICE indexes are high. Moreover, it should be noticed that some of the patients of our sample have EVC valves that generate artifacts. In these cases both ZTE and Atlas show loss of signals but ACmapAtlas has smaller artifacts than ACmapZTE. Further work using Deep learning-based AC will be performed to try to reduce errors in the PET attenuation correction of these kind of patients.Acknowledgements
This research was suported by “Associazione Italiana per la Ricerca sul Cancro”(AIRC) grant number 2018 Id. IG22162. Signa PET/MRI system (GEMS, Wakesha, Wisconsin, USA) used in the present work has been purchased with funding from Italian Ministry of Health.
References
1. Xu, W., et al. The performance of 11C-Methionine PET in the differential diagnosis of glioma recurrence. Oncotarget 2017; 8(53): 91030-91039.
2. Wollenweber, S. D., et al. Evaluation of an atlas-based PET head attenuation correction using PET/CT & MR patient data. IEEE Transactions on Nuclear Science 2013; 60(5): 3383-3390.
3. Wiesinger, F., et al. Zero TE MR bone imaging in the head. Magnetic resonance in medicine 2016; 75(1): 107-114.
4. Ladefoged, C. N., et al. Deep learning based attenuation correction of PET/MRI in pediatric brain tumor patients: evaluation in a clinical setting. Frontiers in neuroscience 2019 (12): 1005.
Figures