1768
Changes in CMR Parameters and Prediction of Cardiac Complications in Thalassemia Major: Fibrosis Tells Us More than Iron.1Fondazione G. Monasterio CNR-Regione Toscana, Pisa, Italy, 2"ARNAS" Civico, Di Cristina Benfratelli, Palermo, Italy, 3Azienda Ospedaliero-Universitaria Ospedali Riuniti "Umberto I-Lancisi-Salesi", Ancona, Italy, 4Policlinico "Paolo Giaccone", Palermo, Italy, 5Presidio Ospedaliero “Giovanni Paolo II”, Lamezia Terme (CZ), Italy, 6Ospedale "V. Cervello", Palermo, Italy, 7Azienda Ospedaliero-Universitaria OO.RR. Foggia, Foggia, Italy, 8Azienda Ospedaliero-Universitaria di Sassari, Sassari, Italy
Synopsis
Seven-hundred and nine patients with thalassemia major who performed a baseline and a 1st follow-up CMR scan after 18 months were followed prospectively in order to evaluate the predictive value of changes in CMR parameters (myocardial iron, biventricular function, and replacement myocardial fibrosis) for cardiac complications. During a mean follow-up of 89.4±33.3 months, cardiac events (heart failure, arrhythmias, and pulmonary hypertension) were recorded in 7.1% of patients. In the univariate Cox regression analysis, cardiac iron clearance and replacement myocardial fibrosis were identified as univariate prognosticators but in the multivariate analysis only myocardial fibrosis remained an independent predictor factor.
Introduction
Cardiovascular magnetic Resonance (CMR) has dramatically changed the clinical practice and improved the prognosis in thalassemia major (TM)1,2.This is the first study evaluating the predictive value of changes in CMR parameters (myocardial iron, function, and fibrosis) for cardiac complications in TM.
Methods
We followed prospectively 709 TM patients (374 females; 29.77±8.53 years) consecutively enrolled in the Myocardial Iron Overload in Thalassemia (MIOT) Network who performed a baseline and a 1st follow up CMR scan after 18 months.Myocardial iron overload (MIO) was measured by multislice multiecho T2* technique3 and atrial dimensions and biventricular function by cine images4. Replacement myocardial fibrosis was detected by late gadolinium enhancement technique5.
Risk classes were defined based on the 4 patterns of MIO from worst to normal. For patients with baseline MIO (at least one segmental T2*<20 ms), improvement was defined as a transition to a better risk class, stabilization as no change in risk class, and worsening as a transition to a worse risk class. For patients without baseline MIO, the worsening was the transition to a worse risk class.
The percentage change was used for continuous variables. For biventricular ejection fractions, improvement was a %change>10%, stabilization a %change between -10% and 10%, and worsening a %change<-10%. For biventricular volumes, LV mass index, and atrial areas, improvement was a % change<-10%, stabilization a % change between -10% and 10%, and worsening a % change>10%.
Replacement myocardial fibrosis was considered absent if not detected in any of the two CMRs and present if detected in at least one examination.
Results
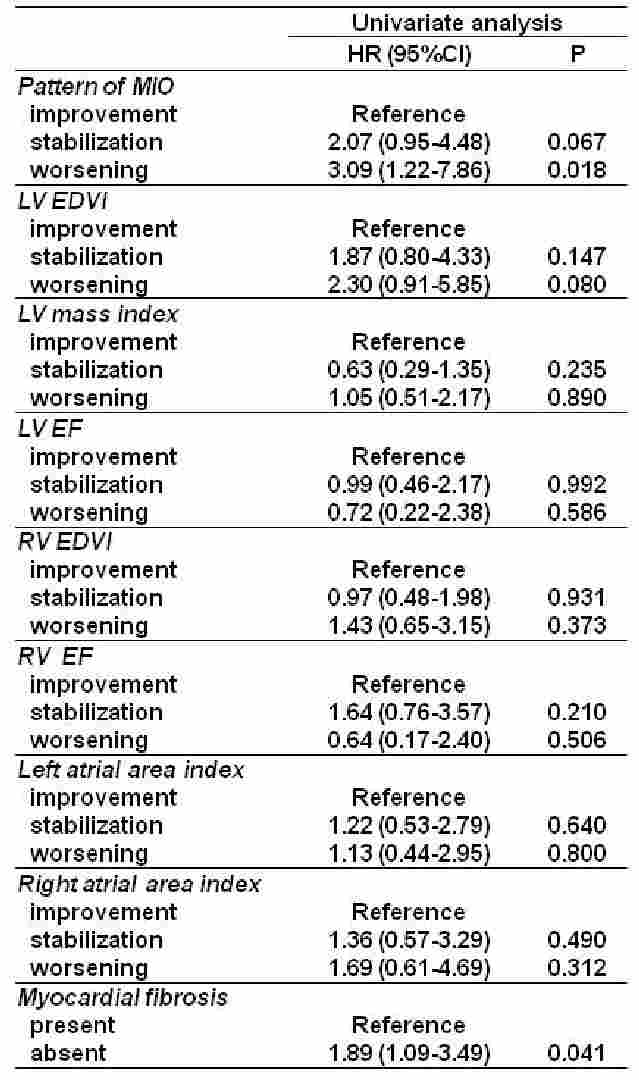
During a mean follow-up of 89.4±33.3 months, cardiac events were recorded in 50 (7.1%) patients: 24 (48%) episodes of heart failure, 24 (48%) arrhythmias (23 supraventricular and 1 hypokinetic), and 2 (4.0%) pulmonary hypertension. Mean time from the 1st follow up CMR to the development of a cardiac complication was 75.31±35.35 months. In the univariate Cox regression analysis, cardiac iron clearance and replacement myocardial fibrosis were identified as univariate prognosticators (Table 1). In the multivariate analysis only myocardial fibrosis remained an independent predictor factor.Conclusions
The presence of replacement myocardial fibrosis at the baseline CMR or developed within 18 months emerges as the strongest long-term predictor for cardiac complications in TM. Our data demonstrate the importance in using the contrast medium for CMR scans in thalassemia patients.Acknowledgements
We thank all the colleagues of the MIOT Network (https://miot.ftgm.it) and all patients for their cooperation.References
1. Modell B, Khan M, Darlison M, Westwood MA, Ingram D, Pennell DJ. Improved survival of thalassaemia major in the UK and relation to T2* cardiovascular magnetic resonance. J Cardiovasc Magn Reson. 2008;10(1):42.
2. Pennell DJ, Udelson JE, Arai AE, et al. Cardiovascular function and treatment in beta-thalassemia major: a consensus statement from the American Heart Association. Circulation. 2013;128(3):281-308.
3. Pepe A, Positano V, Santarelli F, et al. Multislice multiecho T2* cardiovascular magnetic resonance for detection of the heterogeneous distribution of myocardial iron overload. J Magn Reson Imaging. 2006;23(5):662-668.
4. Meloni A, Righi R, Missere M, et al. Biventricular Reference Values by Body Surface Area, Age, and Gender in a Large Cohort of Well-Treated Thalassemia Major Patients Without Heart Damage Using a Multiparametric CMR Approach. J Magn Reson Imaging. 2021;53(1):61-70.
5. Pepe A, Positano V, Capra M, et al. Myocardial scarring by delayed enhancement cardiovascular magnetic resonance in thalassaemia major. Heart. 2009;95:1688-1693.
Figures