1703
Evaluating the impact of respiratory binning strategies on 4D-MRI reconstruction for an MR-Linac1Joint Department of Physics, The Institute of Cancer Research, London, United Kingdom, 2Department of Computing, Imperial College London, London, United Kingdom, 3The Royal Marsden NHS Fundation Trust, London, United Kingdom
Synopsis
In the context of MR-guided radiotherapy, 4D-MRI is of particular interest for lung and abdominal cancer treatment, as it enables quantifying the extent of respiratory motion at the time of treatment, facilitating time-efficient midposition treatments. To reduce long reconstruction times of iterative compressed sensing-based reconstructions involving algorithms, such as XD-GRASP, we used a fast C++ implementation. We evaluated the impact of using overlapping respiratory bins and different self-gating signals on image quality and reconstruction time in multiple patients with and without abdominal compression belts.
Introduction
The MR-Linac offers new combined imaging and treatment opportunities for adaptive radiotherapy by minimizing the delay between MRI acquisition and treatment delivery1. For lung and abdominal cancers, 4D-MRI’s capability to resolve respiratory motion is crucial to track the tumour position through the respiratory cycle2. Radial imaging techniques have been combined with different reconstruction algorithms3, 4 to produce such 4D-MRI with a short acquisition time, but long reconstruction times can be prohibitive in an online adaptive MR-guided radiotherapy workflow. Here we evaluated the impact of respiratory binning strategies on 4D-MRI reconstruction for an MR-Linac.Methods
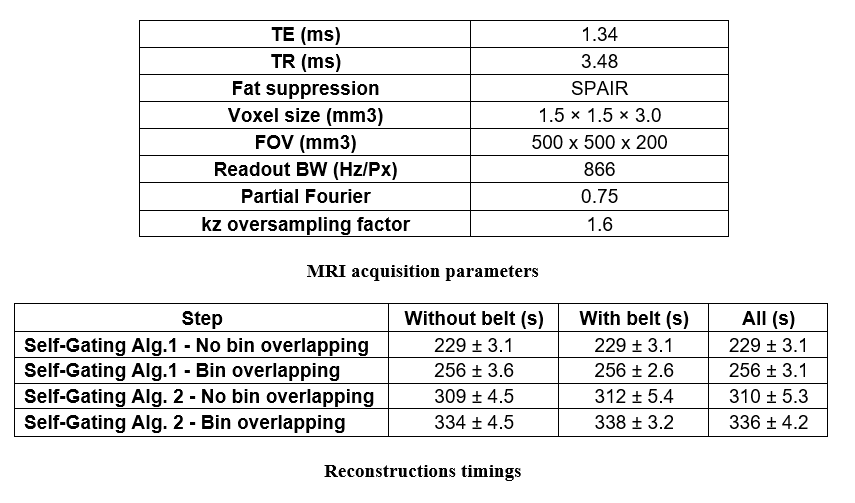
A balanced volumetric radial gradient echo sequence with stack-of-stars readout and golden-angle spacing5 was acquired on a 1.5T MR-Linac system (Unity, Elekta AB, Stockholm) on 4 abdominal cancer patients throughout their radiotherapy treatment. Sequence parameters can be found in Table 1. An asymmetric readout was used to minimize the echo time. 415 samples were acquired for each readout. In total 831 spokes have been obtained. Patients were scanned twice in one session: with and without a compression belt (Figure 1).K-space sample location were corrected using an implementation of the TrACR algorithm6. XD-GRASP was implemented in C++ compiled with g++ 9.3 with MATLAB (MathWorks, Natick, MA) interface and executed on a workstation with an Intel Xeon E5-1660 processor and 128GB of RAM.
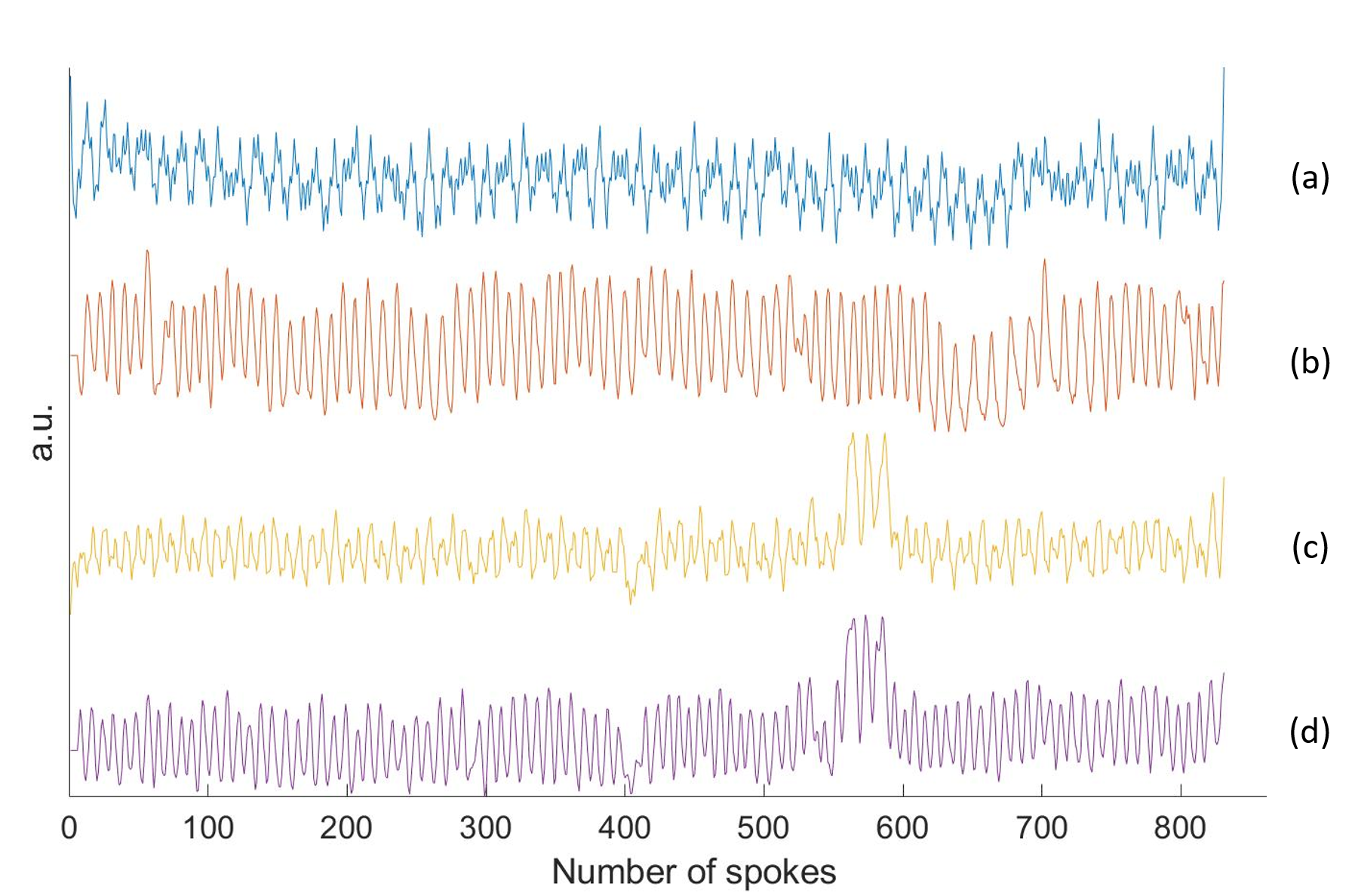
Two different self-gating algorithms were used to determine the respiratory signal. The first algorithm involved a Principal Component Analysis (PCA) on the Fast Fourier Transform (FFT) along kz of the central point of each spoke3 (Algorithm 1), while the second method4 used the magnitude signal for the central points of each spoke through the k-space centre combined with a moving average filter on the k-space data sorted by spoke angle, to account for remaining angle-dependent effects related to B0 inhomogeneity and gradient delays7 (Algorithm 2).
Data were sorted by respiratory signal into 10 respiratory bins either without overlapping or with 50% data overlap between adjacent respiratory bins. Each bin contained the same amount of data.
Results
The durations of the total reconstructions with the different binning strategies are presented in Table 2. The computing time is higher for self-gating algorithm 2 and is also increased if overlapping respiratory bins are used. The overlapping binning with Angle-dependent correction of the angle-dependent delays is therefore the longest reconstruction.Respiratory signals extracted with Algorithm 1 and Algorithm 2 are presented in Figure 2. The Algorithm 1 gives a noisier signal especially if the patient is not wearing a compression belt.
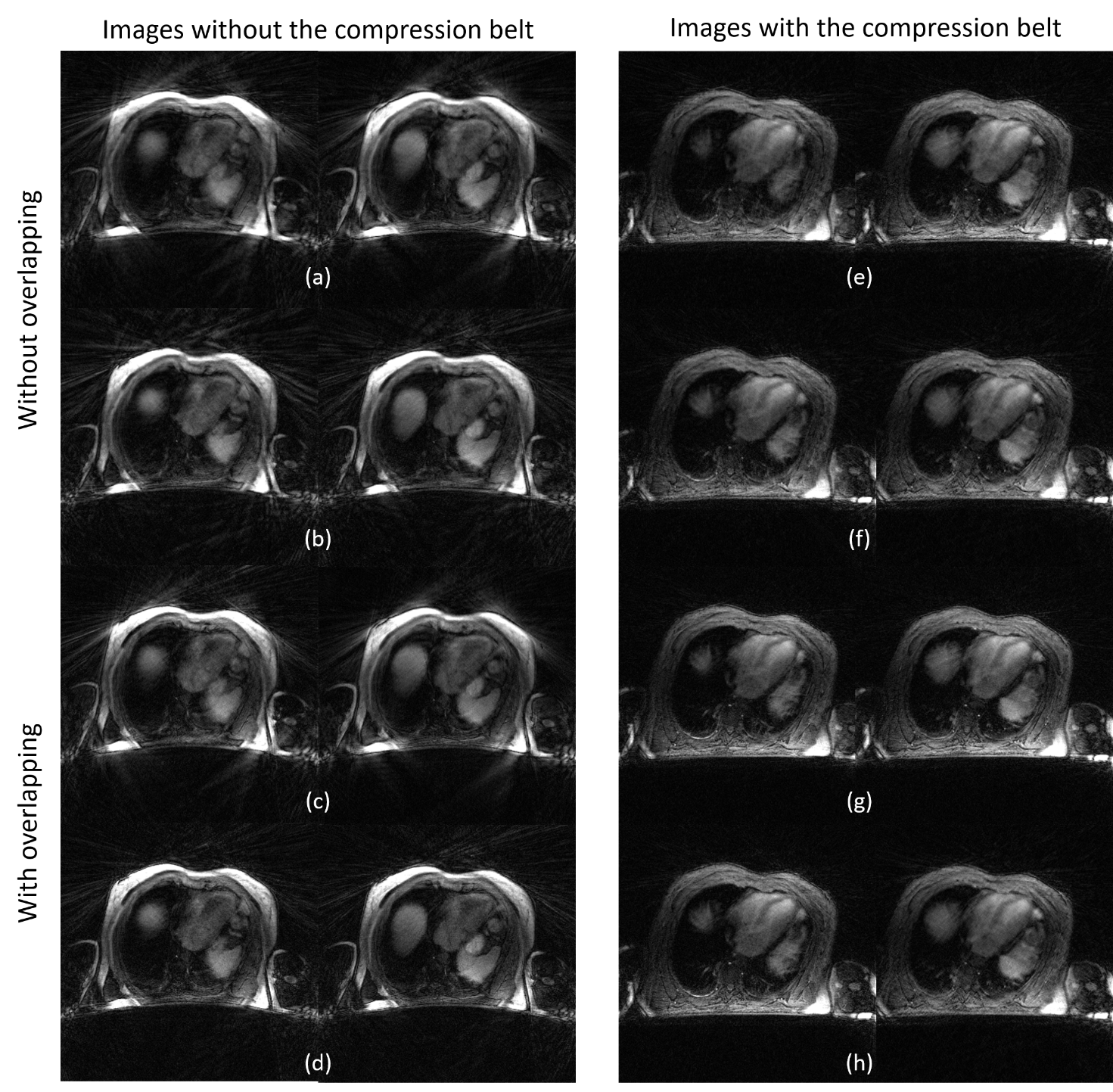
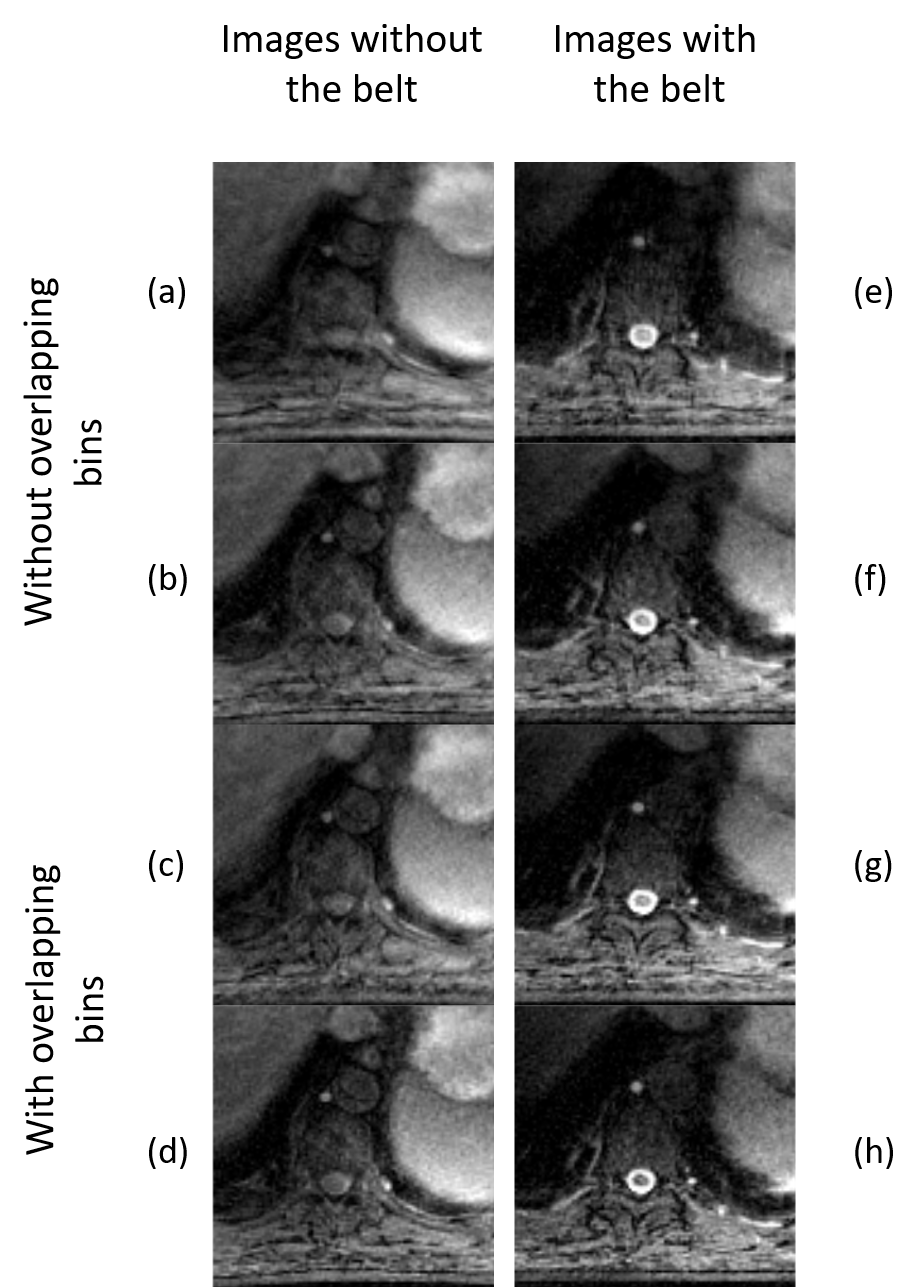
Examples of slices obtained with the combination of the different strategies are given in Figure 3. Images obtained with the compression belt present less noise. The details of the anatomy are more visible with the strategy using overlapping bins and self-gating Algorithm 2. Images are sharper when the patient wears the compression belt.
Discussion and conclusion
Compression belts are used in radiotherapy to suppress large respiratory motion amplitudes, but the remaining motion is still highly relevant for treatment planning. It is often difficult to obtain a good respiratory trace using 4D-CT. Here we showed initial results demonstrating that self-gated respiratory-resolved 4D-MRI techniques can work with abdominal compression as no external reference signal is required. Overlapping respiratory bins can improve image quality without having a major impact on image reconstruction time. We found that a self-gating signal using the magnitude of the k-space centre data was able to better resolve remaining respiratory motion than a kz-projection. 4D-MRI can inform volumetric real-time imaging using techniques such as MR-SIGMA8 on an MR-Linac. The observation that the reconstruction takes longer to converge if self-gating algorithm 2 is used warrants further investigation, including a comparison of the motion amplitudes.In conclusion, we have demonstrated clinically-feasible runtimes for 4D-MRI reconstruction even on outdated hardware which facilitates integration into an MR-Linac workflow. We plan to further accelerate our algorithm by running it on a GPU, which should reduce run times to below 2 minutes9. Further acceleration could be achieved by using deep learning10.
Acknowledgements
No acknowledgement found.References
1. Mickevicius, Nikolai J., and Eric S. Paulson. ‘Investigation of Undersampling and Reconstruction Algorithm Dependence on Respiratory Correlated 4D-MRI for Online MR-Guided Radiation Therapy’ Physics in Medicine & Biology, 62, no. 8 (March 2017): 2910–21. . https://doi.org/10.1088/1361-6560/aa54f2
2. Stemkens, B., E. S. Paulson, and R. H. N. Tijssen. ‘Nuts and Bolts of 4D-MRI for Radiotherapy’ Physics in Medicine & Biology 63, no. 21 (October 2018): 21TR01. https://doi.org/10.1088/1361-6560/aae56d.
3. Feng, Li, Leon Axel, Hersh Chandarana, Kai Tobias Block, Daniel K. Sodickson, and Ricardo Otazo. ‘XD-GRASP: Golden-Angle Radial MRI with Reconstruction of Extra Motion-State Dimensions Using Compressed Sensing’. Magnetic Resonance in Medicine 75, no. 2 (February 2016): 775–88. https://doi.org/10.1002/mrm.25665
4. Rank, Christopher M., Thorsten Heußer, Maria T. A. Buzan, Andreas Wetscherek, Martin T. Freitag, Julien Dinkel, and Marc Kachelrieß. ‘4D Respiratory Motion-Compensated Image Reconstruction of Free-Breathing Radial MR Data with Very High Undersampling’. Magnetic Resonance in Medicine 77, no. 3 (2017): 1170–83. https://doi.org/10.1002/mrm.26206
5. Winkelmann, Stefanie, Tobias Schaeffter, Thomas Koehler, Holger Eggers, and Olaf Doessel. ‘An Optimal Radial Profile Order Based on the Golden Ratio for Time-Resolved MRI’. IEEE Transactions on Medical Imaging 26, no. 1 (January 2007): 68–76. https://doi.org/10.1109/TMI.2006.885337.
6. Ianni, Julianna D., and William A. Grissom. ‘Trajectory Auto-Corrected Image Reconstruction’. Magnetic Resonance in Medicine 76, no. 3 (September 2016): 757–68. https://doi.org/10.1002/mrm.25916.
7. Moussavi, Amir, Markus Untenberger, Martin Uecker, and Jens Frahm. ‘Correction of Gradient-Induced Phase Errors in Radial MRI’. Magnetic Resonance in Medicine 71, no. 1 (January 2014): 308–12. https://doi.org/10.1002/mrm.24643.
8. Kim, Nathanael, Kathryn R. Tringale, Christopher Crane, Neelam Tyagi, and Ricardo Otazo. ’MR SIGnature MAtching (MRSIGMA) with Retrospective Self-Evaluation for Real-Time Volumetric Motion Imaging’ , Physics in Medicine & Biology, 66, no. 21 (October 2021): 215009. https://doi.org/10.1088/1361-6560/ac2dd
9. Marco Barbone, Andreas Wetscherek, Thomas Yung, Uwe Oelfke, Wayne Luk and Georgi Gaydadjiev ‘Efficient Online 4D Magnetic Resonance Imaging’, to be published in 2021 IEEE 33rd International Symposium on Computer Architecture and High Performance Computing (SBAC-PAD) – https://doi.org/10.1109/SBAC-PAD53543.2021.00029
10. Freedman, Joshua N., Oliver J. Gurney-Champion, Simeon Nill, Anna-Maria Shiarli, Hannah E. Bainbridge, Henry C. Mandeville, Dow-Mu Koh, et al. ‘Rapid 4D-MRI Reconstruction Using a Deep Radial Convolutional Neural Network: Dracula’. Radiotherapy and Oncology: Journal of the European Society for Therapeutic Radiology and Oncology 159 (June 2021): 209–17. https://doi.org/10.1016/j.radonc.2021.03.034.
Figures