1669
Accuracy of left ventricular function measurements using retro-gated real-time cine bSSFP cardiovascular magnetic resonance1MRC, London Institute of Medical Sciences, Imperial College London, London, United Kingdom, 2National Heart, Lung, and Blood Institute, National Institute of Health, Bethesda, MD, United States, 3MRC, London Institute of Medical Sciences, UKRI, London, United Kingdom
Synopsis
Cardiac magnetic resonance with a retrospective ECG-gated breath-hold cine stack is the reference standard for assessing LV volumes, however this technique is unsuitable for patients who cannot hold their breath or suffer arrhythmia. A potential solution is a “retro-gated” real-time sequence which is prospectively triggered to acquire 120 frames over multiple heartbeats in each slice. Images from a beat most closely matching the median beat length for the entire stack are then temporally interpolated to 30 output phases for each slice. This retro-gated method showed good agreement with the reference standard sequence in a cohort of healthy volunteers.
Introduction
Accurate left ventricular (LV) volumes play an important role in the management of cardiovascular disease. Standard cardiac magnetic resonance (CMR) with a retrospective electrocardiogram (ECG)-gated breath-hold cine is the reference standard for assessing LV volumes1. This method segments the k-space for each cardiac phase across multiple heartbeats and assumes that all these heartbeats are the same duration. However, this technique is not suitable when there are excessive beat-to-beat variations such as arrhythmia or when patients are unable to hold their breath2.For these patients a prospectively ECG-triggered real-time (RT) technique is often used3, where the k-space for each cardiac phase is acquired in a single heartbeat, normally at the expense of spatial and temporal resolution4. Two drawbacks of ECG-triggered RT are that (1) the entire cardiac cycle is not covered, meaning end-diastolic volume (EDV) and ejection fraction (EF) may be underestimated5, and (2) although each slice is triggered from an R wave, the beat-to-beat variations can mean that the frame at which end-systole is captured can differ from slice to slice. This makes automated volumetric analysis impossible and manual analysis challenging.
A potential solution is a “retro-gated” RT sequence, where at each slice an R wave triggers the acquisition lasting 4 seconds to acquire 120 frames. This acquisition window covers ~4 heart beats, given a typical heart rate of 60bpm. The most consistent heart beat is then chosen across all slices by computing the median R-R interval for all acquired heart beats and selecting for each beat the best closest to mean, while excluding beats preceded by short beats. The images acquired in this best heart beat are then temporally interpolated to 30 output phases during Gadgetron reconstruction resulting in the “retro-gated” real-time output covering the entire cardiac cycle for each slice.
The aim of this study was to investigate the accuracy of the LV volume measurements derived from this retro-gated RT sequence in a cohort of healthy volunteers in sinus rhythm compared to the reference standard retrospective ECG-gated breath-hold sequence.
Method
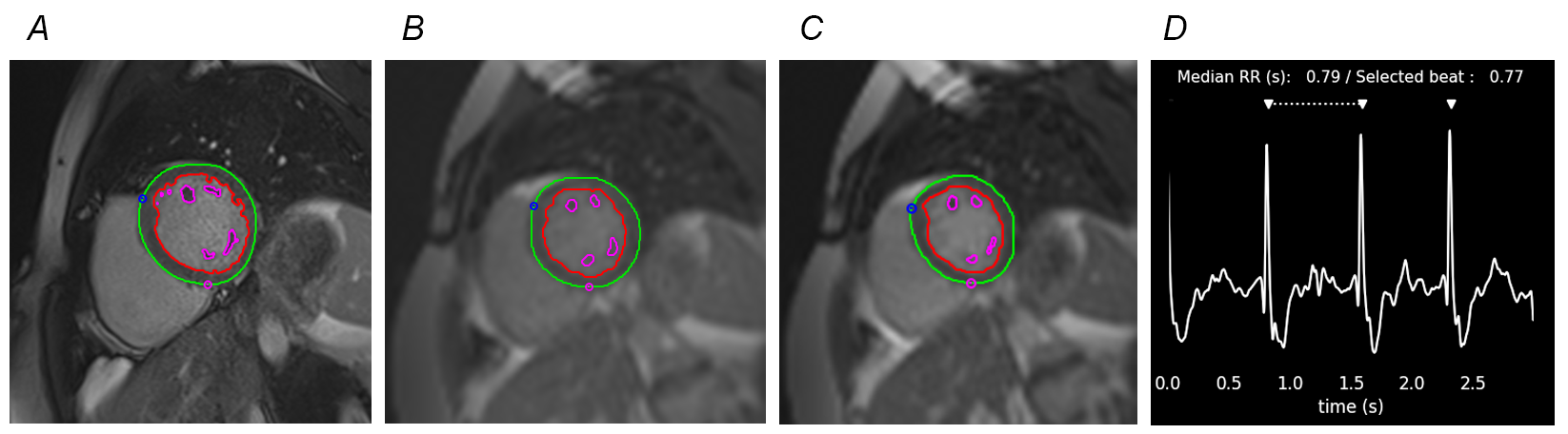
CMR studies were performed on 24 healthy volunteers (mean age: 50y +/-14y) using a 1.5T scanner (MAGNETOM Aera, Siemens Healthineers, Erlangen, Germany) and the 60-channel cardiac coil. A left ventricular short-axis cine stack (LVSA) using a 2D balanced steady-state free precession (bSSFP) was acquired on each subject by three methods: (1) the reference breath-hold retrospectively-gated segmented sequence (bSSFPSBH), (2) a standard prospectively triggered breath-hold real-time sequence (bSSFPRTP) and (3) the “retro-gated” prospectively triggered free-breathing real-time sequence (bSSFPRTRG). Sequence parameters are summarised in Figure 1.Quantitative analysis of EDV, end-systolic volume (ESV), stroke volume (SV) and EF was performed by an experienced CMR technologist using CVI42 (v5.13.5, Circle Cardiovascular Imaging, Calgary, Canada). For each of the three LVSA sequences the epicardial and endocardial contours were automatically traced and manually corrected if necessary. The end-systolic and end-diastolic phases were automatically detected, based on the smallest and largest LV volumes over the entire cardiac cycle (Figure_2).
The quantitative results were compared using a linear mixed model ANOVA with post-hoc pairwise comparison. A p-value of less than 0.05 was considered statistically significant. Correlation and Bland-Altman analysis was performed to compare the quantitative measures for each sequence.
Results
All 24 participants had a regular sinus rhythm with the mean heart rate across all participants 63 ± 9 bpm. There was no statistically significant difference between the bSSFPSBH, bSSFPRTP and bSSFPRTRG for all LV volume measurements (Figure_3).There was a significant correlation between the bSSFPRTRG and bSSFPSBH for EDV (R2=0.87, p<0.05), ESV (R2=0.78, p<0.05), SV (R2=0.84, p<0.05) and EF (R2=0.56, p<0.05). There was also a significant correlation between the bSSFPRTP and bSSFPSBH for EDV (R2=0.89, p<0.05), ESV (R2=0.84, p<0.05), SV (R2=0.74, p<0.05) and EF (R2=0.40, p<0.05) (Figure_4).
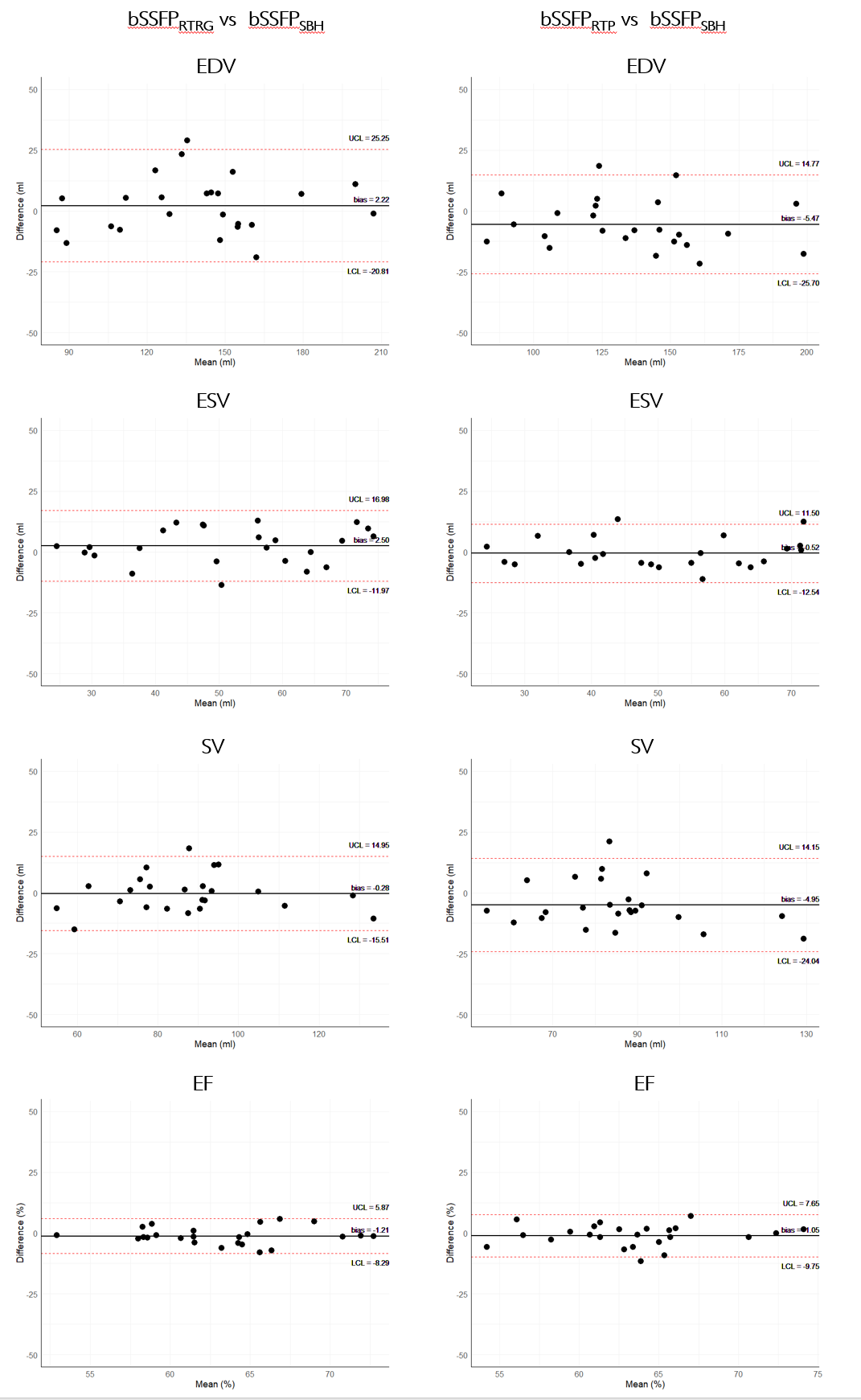
Bland-Altman analysis (Figure_5) revealed a mean bias between the bSSFPRTRG and bSSFPSBH for EDV of 2.2mls (95% LoA, -20.8mls to 25.3mls), for ESV of 2.5mls (-11.9mls to 16.9mls), for SV of -0.3mls (-15.5mls to 14.9mls) and for EF of -1.2% (-8.3% to 5.9%). The mean bias between the bSSFPRTP and bSSFPSBH for EDV was -5.5mls (95% LoA, -25.7mls to 14.8mls), for ESV was -0.5mls (-12.5mls to 11.5mls), for SV was –4.9mls (-24.0mls to 14.2mls) and for EF was -1.1% (-9.8% to 7.7%).
Discussion
The bSSFPRTRG showed high agreement for the volumetric analysis of the LV when compared to the current reference standard multi-breath-hold cine. As this technique is able to image the entire cardiac cycle it did not underestimate the EDV and EF as traditional bSSFPRTP did (mean bias 2.2ms vs -5.5ms).The consistent number of reconstructed cardiac phases in the bSSFPRTRG ensured that analysis was straightforward as the end-systolic frame was the same for all slices in the LVSA. Although the spatial resolution of both the bSSFPRTRG and bSSFPRTP was less than that of the bSSFPSBH it did not hinder the automated delineation of endo- and epicardial borders nor the automatic detection of end-diastole and end-systole.
Conclusion
Retro-gated RT CMR provides an accurate method for volumetric analysis of the LV and has the potential to provide a viable alternative to the standard retrospective-gated breath-hold method in patients who are unable to hold their breath or who suffer from arrhythmia.Acknowledgements
No acknowledgement found.References
1. Alfakih K, Plein S, Thiele H, Jones T, Ridgway JP, Sivananthan MU. Normal human left and right ventricular dimensions for MRI as assessed by turbo gradient echo and steady-state free precession imaging sequences. J Magn Reson Imaging. 2003;17:323–9. https://doi.org/10.1002/jmri.10262
2. Ferreira, P.F., Gatehouse, P.D., Mohiaddin, R.H. et al. Cardiovascular magnetic resonance artefacts. J Cardiovasc Magn Reson 15, 41 (2013). https://doi.org/10.1186/1532-429X-15-41
3. Allen, B.D., Carr, M.L., Markl, M. et al. Accelerated real-time cardiac MRI using iterative sparse SENSE reconstruction: comparing performance in patients with sinus rhythm and atrial fibrillation. Eur Radiol 28, 3088–3096 (2018). https://doi.org/10.1007/s00330-017-5283-0
4. Setser RM, Fischer SE, Lorenz CH. Quantification of left ventricular function with magnetic resonance images acquired in real time. J Magn Reson Imaging. 2000 Sep;12(3):430-8. https://doi:10.1002/1522-2586(200009)12:3<430::aid-jmri8>3.0.co;2-v. PMID: 10992310
5. Kido, T., Kido, T., Nakamura, M. et al. Compressed sensing real-time cine cardiovascular magnetic resonance: accurate assessment of left ventricular function in a single-breath-hold. J Cardiovasc Magn Reson 18, 50 (2016). https://doi-org.iclibezp1.cc.ic.ac.uk/10.1186/s12968-016-0271-0
Figures
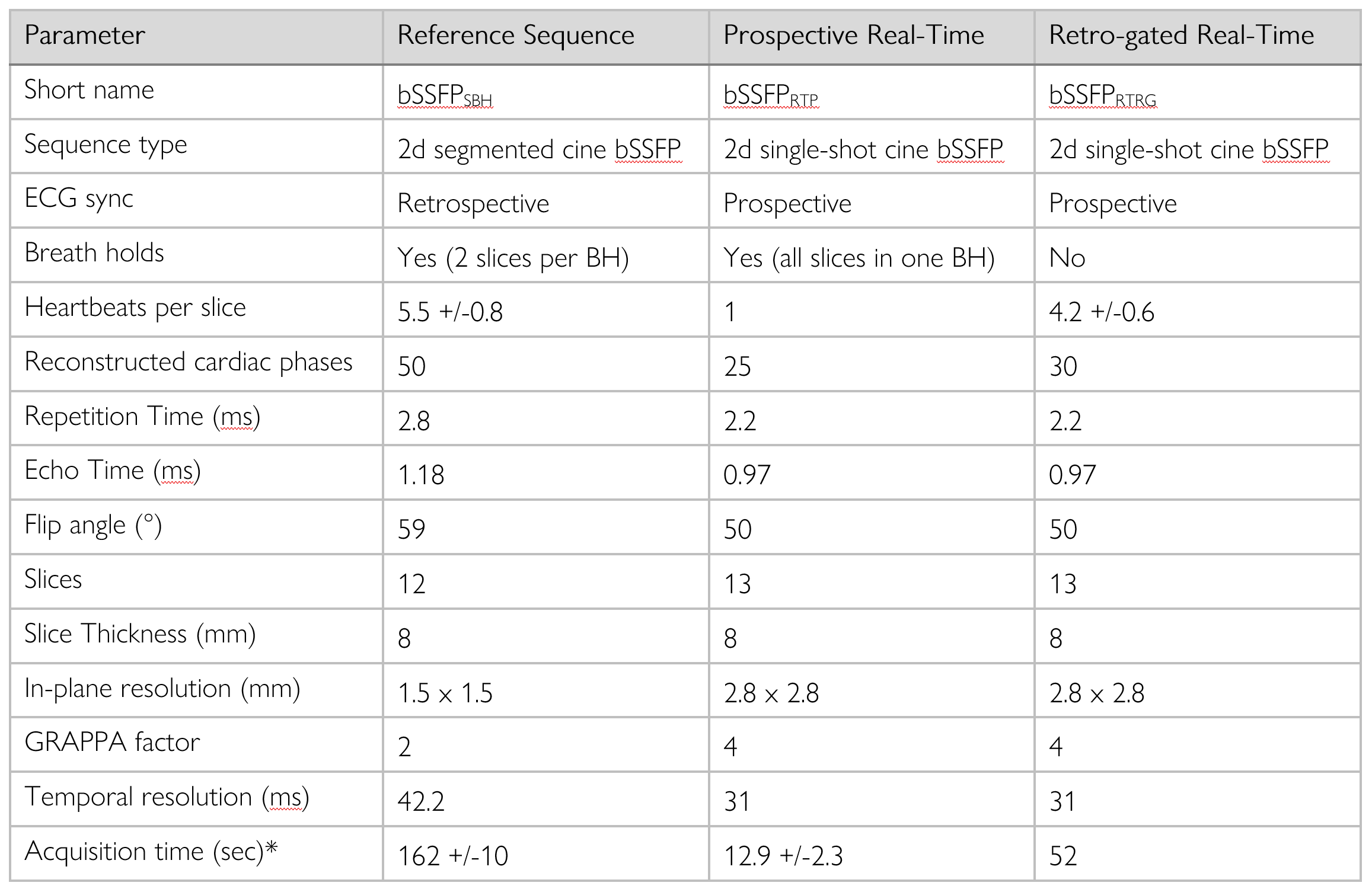
Acquisition parameters for reference standard sequence (bSSFPSBH), Prospective Real-Time sequence (bSSFPRTP) and Retro-gated Real-Time sequence (bSSFPRTRG).
*Acquisition time for entire stack including breaks between breath holds