1661
Texture Analysis Identifies Significant Pattern Differences in Pediatric Heart Transplant Recipients with and without Acute Rejection
Margaret Samyn1, Ke Yan2, Kristen George-Durrett3, Justin Godown3, Kimberly Crum3, Maryanne Christ4, Kak-Chen Chan4, Kak-Chen Chan4, David Bearl3, Debra Dodd3, Lazaro Hernandez4, Jonathan Soslow3, and Bruce Damon5
1Pediatrics, Medical College of Wisconsin, Milwaukee, WI, United States, 2Biostatistics, Medical College of Wisconsin, Milwaukee, WI, United States, 3Pediatrics, Division of Pediatric Cardiology, Vanderbilt University Medical Center, Nashville, TN, United States, 4Pediatric Cardiology, Joe DiMaggio Children’s Hospital at Memorial Healthcare System, Hollywood, FL, United States, 5Stephens Family Clinical Research Institute Carle Foundation Hospital, Urbana, IL, United States
1Pediatrics, Medical College of Wisconsin, Milwaukee, WI, United States, 2Biostatistics, Medical College of Wisconsin, Milwaukee, WI, United States, 3Pediatrics, Division of Pediatric Cardiology, Vanderbilt University Medical Center, Nashville, TN, United States, 4Pediatric Cardiology, Joe DiMaggio Children’s Hospital at Memorial Healthcare System, Hollywood, FL, United States, 5Stephens Family Clinical Research Institute Carle Foundation Hospital, Urbana, IL, United States
Synopsis
Acute rejection (AR) continues to cause significant morbidity and mortality in pediatric heart transplant recipients (PHTx). Endomyocardial biopsy is the standard-of-care for diagnosis of AR, but it is invasive and associated with morbidity and mortality and can miss patchy AR. Cardiac magnetic resonance (CMR) was performed using parametric mapping and novel texture analysis to detect patterns of myocardial edema and fibrosis. Patients with AR had significant differences in texture analysis compared with patients without AR. CMR with texture analysis has potential as a non-invasive method for detection of AR in PHTx.
Introduction
Despite advances in care for pediatric heart transplant recipients (PHTx), acute rejection (AR) remains a significant cause of morbidity and mortality. Endomyocardial biopsy (EMB) is the standard clinical method for diagnosing AR, but EMB is associated with morbidity, mortality, patient anxiety, and high medical costs. AR is often a patchy process and EMB can only access the right ventricular endomyocardial surface of the septum. Therefore, a non-invasive method to screen for AR would be of significant value, as it may be used to predict who needs EMB. Cardiac magnetic resonance (CMR) parametric mapping (native T1, T2, and extracellular volume) can detect extracellular matrix expansion associated with AR. However, CMR analyses focus on the lower order moments of the distribution of voxel values across a tissue plane or region, such as the central tendency or variance. Texture analyses, on the other hand, quantify the relationships of signal intensities across adjacent image voxels, allowing for quantification of spatial patterns such as diffusiveness, patchiness, etc. at voxel-level resolution. We hypothesized that texture analyses of CMR parametric mapping can detect evidence of AR in PHTx.Methods
Twenty-nine PHTx recipients were enrolled at two sites. Patients were enrolled either within 5 days of AR diagnosis or at surveillance catheterization. There were 10 unique episodes of biopsy+AR. Subjects underwent CMR with contrast, including modified Look-Locker inversion recovery (MOLLI) performed pre- and 15 minutes post-contrast administration in two basal short axis planes, two mid-LV short axis planes, and a 4-chamber (4-ch) plane. T2mapping was also performed in the same slice locations. ECV maps were created using native and post-contrast T1 maps and a same-day hematocrit. Standard volume and function analysis was performed using Qmass (Medis). Late gadolinium enhancement (LGE) semi-quantification was performed using a 5 standard deviation technique. The ECV, native T1, post-contrast T1, and T2 maps from AR+ and AR– patients (Figure 1) were analyzed using texture analyses in a purpose-built matlab program. First, the LV epicardial border and septum were hand-defined. The chamber was segmented using k-means clustering, and partial volume artifacts along the LV endocardial border were removed. The resulting maps were characterized using typical descriptive statistics and measures derived from the gray-level co-occurrence (GLCM) and gray-level run-length (GLRLM) matrices.Results
The median age of subjects was 16 years with interquartile range (IQR) of 13-18 years. The median left ventricular ejection fraction (LVEF) was 59% with IQR 55%-64%. LVEF was decreased in subjects with AR as compared to those without AR (51% IQR[42,56] vs 61% IQR[59,64], p<0.001). Approximately 55% of subjects had LGE and there was no difference in LGE presence or quantification between AR+ and AR– groups. While 44/300 possible comparisons showed statistical significance, a common finding was that the autocorrelation value was elevated (reflecting less randomness to adjacent voxel values): Biopsy+AR patients had significantly higher autocorrelation values for ECV, native T1, and T2 in the 4-chamber and base planes. Also, biopsy+AR patients had elevated high gray-level run-length emphasis values for native and post-contrast T1. They had higher ECV in the mid- and base- short-axis views and increased T2 at the mid-short axis plane. These findings reflect a tendency toward long runs of interconnected voxels having high values for the measure of interest. Lastly, several cluster metrics, reflecting asymmetry to the distribution of values, were elevated in biopsy+AR patients.Conclusions
Multiple texture properties – which reflect the structured presence of connected voxels having high values for the measure of interest – offer potential for diagnostic classification for the presence or absence of AR in PHTx recipients. Often, these abnormalities occurred in regions inaccessible by endomyocardial biopsy.Acknowledgements
No acknowledgement found.References
No reference found.Figures
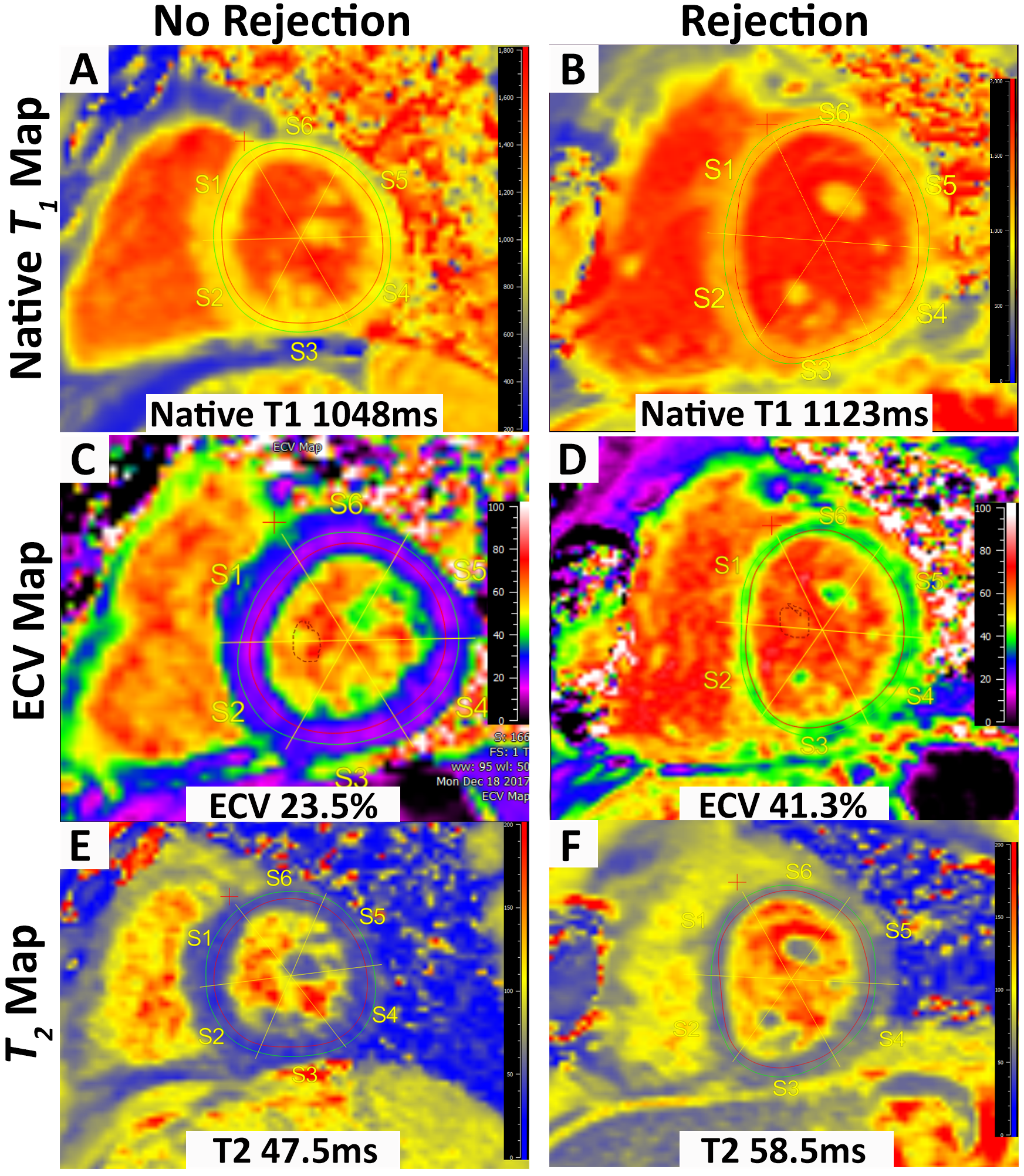
Figure 1. Example Parametric Maps. A,C,E: Native T1, ECV, and T2 maps in an AR– PHTx patient. B,D,E: PHTx patient with AR.
DOI: https://doi.org/10.58530/2022/1661