1654
Free-breathing pseudo-golden-angle bSSFP cine cardiac MRI for evaluation of biventricular function in patients with congenital heart disease1Diagnostic and interventional radiology, University Hospital Bonn, Bonn, Germany, 2Philips GmbH DACH, Hamburg, Germany, 3Pediatric Cardiology, University Hospital Bonn, Bonn, Germany
Synopsis
Cardiac MRI is currently the standard imaging modality for patients with congenital heart disease (CHD). However, the requirement for breath holds remains a big challenge in clinical practice and image quality is often significantly degraded by respiratory motion artifacts. We employed respiratory-triggered pseudo-golden-angle bSSFP imaging for free-breathing cine MRI and compared cardiac volumetry, function, and image quality with the standard breath hold technique. The proposed method showed good agreement with comparable diagnostic image quality and advantage in patients with limited breath hold capability. These demonstrated promise for a wider clinical routine application in patients with CHD.
Introduction
IntroductionCardiac MRI is the modality of choice when it comes to imaging in congenital heart disease (CHD) patients as it allows for analysis of ventricular function and avoids ionizing radiation.1 Current routine cardiac MRI cine images require breath holds (BH) during long acquisitions such as axial or short axis cine sequences to generate diagnostic data. In ideal settings, patients are able to accommodate the long acquisition times and BH allowing for sufficient temporal and spatial resolution. When BH cannot be sufficiently performed, imaging quality suffers, in worst cases producing non-diagnostic data leading to a repeat of the examination and thus prolonged acquisition times. This can lead to difficult examination conditions in CHD patients who also often suffer a physiologically elevated heart rate, and potential anxiety. Current approaches to compensate for this require examinations under sedation leading to risks associated with anesthesia. However, multi-slice respiratory-triggered pseudo-golden-angle bSSFP cine cardiac MRI might allow for data acquisition without the need for respiratory suspension by utilizing golden angle radial k-space sampling.2,3
Methods
Twenty-five CHD patients (mean age 24±9 years, 17 males) underwent routine cardiac MRI including standard breath-hold (BH) 4-chamber and short axis (SA) bSSFP cine imaging. For free-breathing (FB) respiratory-triggered pseudo-golden-angle bSSFP cine 4-chamber und SA views were performed after obtaining patient consent. The FB sequences were respiratory belt-triggered, with the expiratory phase defined as the triggering point with 150 ms duration for start-up excitation to drive the magnetization to steady state, before commencing the ECG-gated acquisition.3 Radial pseudo-golden-angle k-space sampling was applied for image acquisition using segmented balanced SSFP turbo-field-echo (bTFE) pulse sequences with retrospective ECG gating.2 The FB and BH sequences were quantitively analyzed for left and right ventricular volumes, function, signal to noise ratio (SNR), and estimated contrast to noise ratio (CNR). 4-chamber and SA images of both, the BH and FB sequences, were qualitatively compared for image quality by two independent radiologists regarding three imaging criteria (contrast, endocardial edge definition, and artefacts) on a 5 point numeric rating scale (5 excellent, 4 good, 3 adequate, 2 poor, 1 non-diagnostic). Statistical analysis was carried out using a two tailed paired t-Test and Bland-Altman analysis for direct comparisons. Inter-user agreement was compared using interclass correlation.
Results
No statistical differences were found between the BH and FB sequences regarding intraventricular septum thickness in diastole (IVSD, 7.4±2.0 mm vs 7.4±1.8 mm, p=.71), left ventricular ejection fraction (LVEF, 56.4±10.3 % vs 55.7±8.5 %, p=.57), left ventricular end diastolic volume (LVEDV, 176.3±65.8 ml vs 173.9±66.6 ml, p=.47), left ventricular end diastolic volume index (LVEDVi, 99.6±34.1 ml/m2 vs 99.8±35.9 ml/m2, p=.90), right ventricular ejection fraction (RVEF, 49.3±9.1 % vs 49.3±10.8 %, p=.93), right ventricular end diastolic volume (RVEDV, 186.6±75.8 ml vs 184.0±56.3 ml, p=.81), and right ventricular end diastolic volume index (RVEDVi, 104.6±37.1 ml/m2 vs 103.3±25.7 ml/m2, p=.83) (Fig. 1). The average acquisition time for a FB 4-chamber sequence was 1.2 minutes, 2.8 times longer than a BH 4-chamber with 0.41 minutes. Similarly, FB SA sequences took around 9.22 minutes to acquire compared to 4.26 minutes for BH (ratio of 2.2). On average, the BH 4-chamber and SA scored 13.9±1.8 and 14.7±1.0 points out of 15 regarding subjective image quality compared to 13.4±1.8 and 13.6±1.6 points for the FB HLA and SA, respectively. The interclass correlation coefficient was good with agreements of 0.84 (BH 4-chamber view), 0.78 (FB 4-chamber view), 0.86 (BH short axis), and 0.78 (FB short axis). The BH SA sequence demonstrated an average SNR and estimated CNR of 1.0±0.7 and 124.1±35.5, respectively, compared to 0.4±0.3 and 91.7±45.7 for the FB SA.
Discussion
Free-breathing multi-slice respiratory-triggered pseudo-golden-angle bSSFP cine imaging performed nearly identical to currently available BH sequences regarding left and right ventricular volumetry and function (Fig. 2). Regarding imaging quality, the images produced by FB sequences suffer slightly from radial acquisition artefacts which was also reflected in lower subjective image quality scores (14.7±1.0 vs 13.6±1.6 points). These artefacts are an inherent part of the acquisition technique, currently there exist no known algorithms to correct for these radial artefacts, but as the volumetric data shows, they do not interfere with quantitative image analysis (no significant difference between FB and BH sequences for IVSD, LVEF, LVEDV, LVEDVi, RVEF, RVEDV, or RVEDVi). They also demonstrated a lower SNR (0.4±0.3 vs 1.0±0.7) and CNR (91.7±45.7 vs 124±35.5). However, the benefit of this technique becomes evident in cases where patients were unable to perform breath-holds (Fig. 3), leading to non-diagnostic images and repeated examinations. In these cases, FB sequences were able to salvage the examination leading to diagnostic data, where BH sequences failed. In general, image quality of FB sequence were not hampered by severe motion artifacts and might be a reliable imaging option in CHD patients with limited breath holding capacities.
Conclusion
Free-breathing multi-slice respiratory-triggered pseudo-golden-angle bSSFP cine imaging produce images subjectively slightly inferior to normal BH sequences but remain diagnostic with no difference regarding IVSD, right and left EF, EDV, and EDVi. When patients were unable to adequately suspend respiration, FB sequences were able to produce diagnostic images where BH sequences failed.
Acknowledgements
No acknowledgement found.References
(1) Valsangiacomo Buechel, E. R.; Grosse-Wortmann, L.; Fratz, S.; Eichhorn, J.; Sarikouch, S.; Greil, G. F.; Beerbaum, P.; Bucciarelli-Ducci, C.; Bonello, B.; Sieverding, L.; Schwitter, J.; Helbing, W. A.; Galderisi, M.; Miller, O.; Sicari, R.; Rosa, J.; Thaulow, E.; Edvardsen, T.; Brockmeier, K.; Qureshi, S.; Stein, J. Indications for cardiovascular magnetic resonance in children with congenital and acquired heart disease: an expert consensus paper of the Imaging Working Group of the AEPC and the Cardiovascular Magnetic Resonance Section of the EACVI. European heart journal. Cardiovascular Imaging 2015, 16 (3), 281–297. DOI: 10.1093/ehjci/jeu129  . Published Online: 17-Feb-15.
. Published Online: 17-Feb-15.
(2) Kajita, K.; Goshima, S.; Noda, Y.; Kawada, H.; Kawai, N.; Okuaki, T.; Honda, M.; Matsuo, M. Thin-slice Free-breathing Pseudo-golden-angle Radial Stack-of-stars with Gating and Tracking T1-weighted Acquisition: An Efficient Gadoxetic Acid-enhanced Hepatobiliary-phase Imaging Alternative for Patients with Unstable Breath Holding. Magnetic Resonance in Medical Sciences 2019, 18 (1), 4–11. DOI: 10.2463/mrms.mp.2017-0173 . Published Online: 09-Mar-18.
(3) Krishnamurthy, R.; Pednekar, A.; Atweh, L. A.; Vogelius, E.; Chu, Z. D.; Zhang, W.; Maskatia, S.; Masand, P.; Morris, S. A.; Krishnamurthy, R.; Muthupillai, R. Clinical validation of free breathing respiratory triggered retrospectively cardiac gated cine balanced steady-state free precession cardiovascular magnetic resonance in sedated children. J Cardiovasc Magn Reson 2015, 17 (1), 1. DOI: 10.1186/s12968-014-0101-1 . Published Online: 14-Jan-15.
Figures
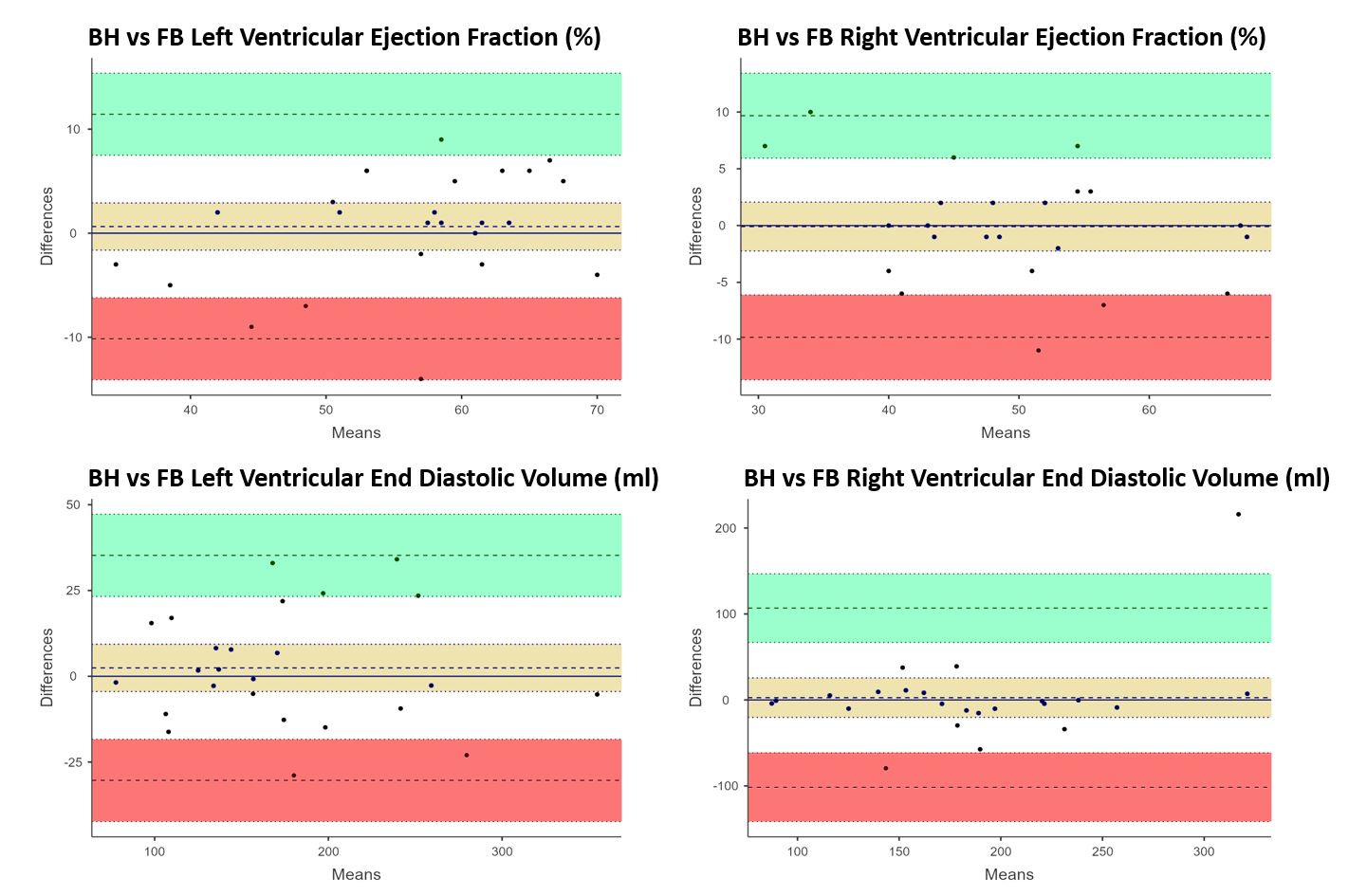
Fig. 1 Bland-Altman plots demonstrating good agreement comparing left ventricular ejection fraction, right ventricular ejection fraction, left ventricular end diastolic volume, and right ventricular end diastolic volume between breath hold (BH) and free breathing (FB) sequences.
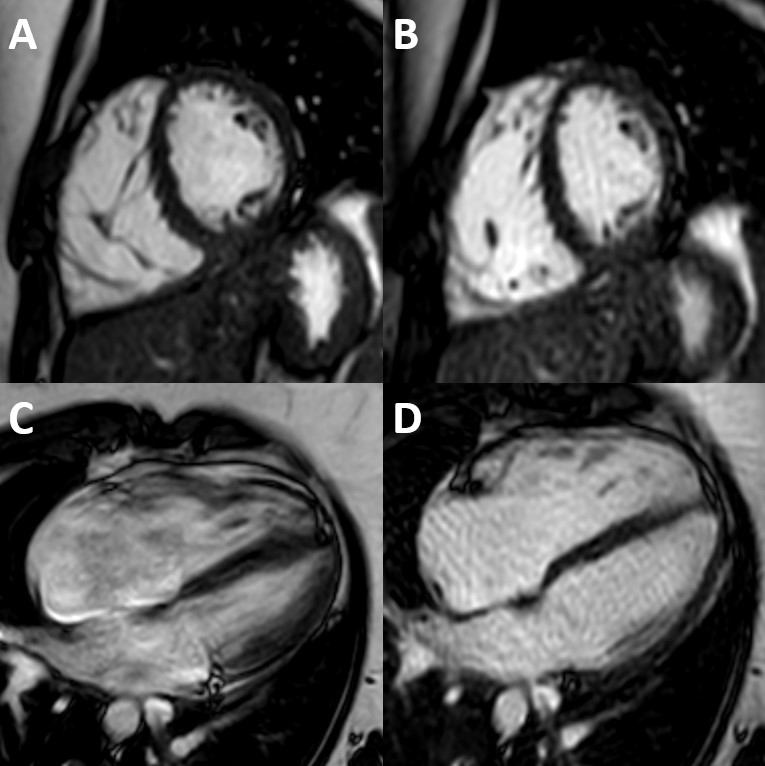
Fig. 2 Comparison of short axis views in balanced steady-state free precession (bSSFP) breath hold (A) and pseudo-golden angle radial sampling bSSFP free breathing (B) sequences as well as 4-chamber views breath hold (C) and free breathing (D) sequences in a 24-year-old female suffering from a type 2 atrial septum defect. While both (A) and (B) demonstrate comparable images, (C) suffers from motion artefacts and a lack of endocardial edge definition while (D) allows for diagnostic images.
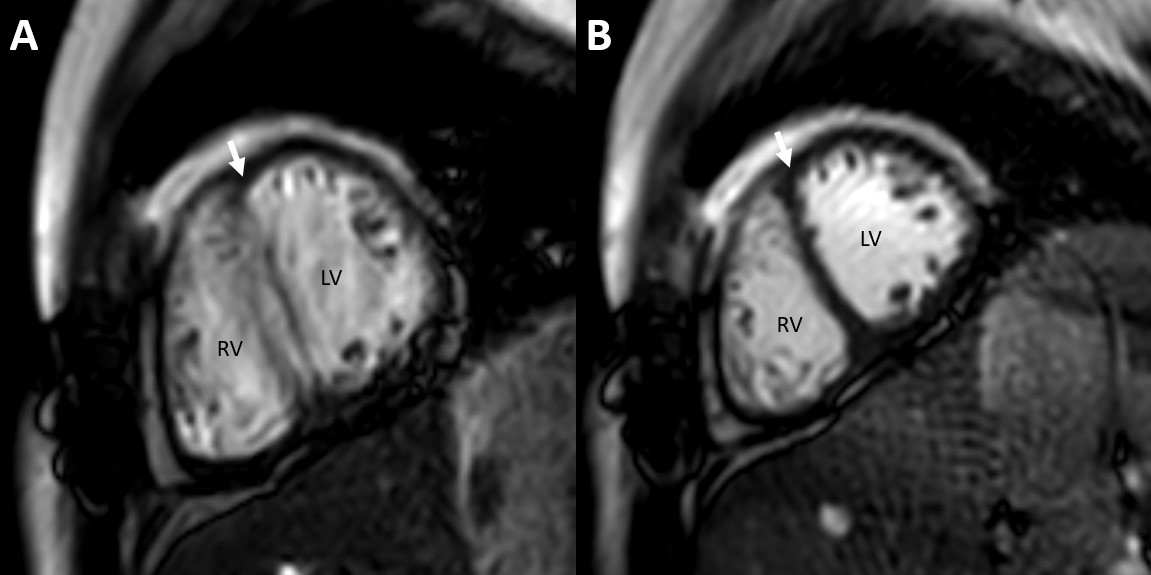
Fig. 3 Comparison of short axis views in balanced steady-state free precession (bSSFP) breath hold (A) and bSSFP pseudo-golden angle radial sampling free breathing (B) short axis views of the right (RV) and left ventricles (LV) in a 26-year-old male. Motion artefacts obscure the septal border (arrow) in the breath hold sequence (A) while the free breathing sequence demonstrates sharp endocardial contours (B).