1653
Enabling Pilot Tone cardiac triggering for complete cardiac examinations using an RF calibration procedure
Peter Speier1, Yan Tu Huang2, Carmel Hayes1, Randall Kroeker1, Manuela Rick1, Michael Schwertfeger3, and Mario Bacher1
1Siemens Healthcare, Erlangen, Germany, 2Siemens Healthcare, Shenzen, China, 3ASTRUM IT GmbH, Erlangen, Germany
1Siemens Healthcare, Erlangen, Germany, 2Siemens Healthcare, Shenzen, China, 3ASTRUM IT GmbH, Erlangen, Germany
Synopsis
Contactless cardiac triggering using Pilot Tone was initially demonstrated for steady-state triggered cine-type sequences that, per definition, are performed with continuous, uniform RF pulses. Here we describe a method that stabilizes Pilot Tone cardiac triggering in the presence of RF artefacts, thereby allowing for pilot tone triggering of complete cardiac MR examinations with a range of sequence flavors including those applying RF pulses intermittently. The method uses an additional RF calibration measurement and avoids the RF artefact subspace in a PCA-based multi-channel coil combination calculation. Signal examples at 1.5T demonstrate effective RF suppression.
Motivation
Cardiac examinations require a trigger signal source, the clinical gold standard being ECG. Here we describe an alternative workflow and processing pipeline for contactless triggering based on Pilot Tone magnetic navigation [1-3]. PT cardiac triggering (PTC) has been previously described for measurements with continuous RF trains (e.g., Cine) [4-6]. To enable PTC for measurements with varying RF one must suppress artefacts in the PT signal caused by the RF pulses. This approach has already been tested for the standard clinical field strengths of 1.5 and 3T [7,8].Methods
Cardiac product sequences were modified to enable selection of the new trigger signal source, to play out RF calibration pulse trains, and to provide modified PT processing modules for volunteer measurements on several 1.5T scanners with integrated PT generation and detection (MAGNETOM Sola and Altea, Siemens Healthcare, Erlangen, Germany).RF Calibration sequence
A train of 40 high power RF pulses 100kHz off resonance with pulse spacing 4ms and typical bSSFP parameters (1ms, 70°, SINC, BWT 2) is repeated four times with gaps of 2s. The RF pulses carry IDs that identify the beginning and end of the RF calibration block and its constituent RF trains.
Processing
PTC raw data is processed in two threads: in a real-time processing thread for inline per-sample processing, and in a background thread with lower priority for extensive calculations.
Real-time thread: per-sample pipeline
The inline thread receives and processes two inputs:
- a continuous PT raw data stream of complex valued PT samples for every active channel with a sample rate of 2kHz. Each sample carries a time stamp and a validity flag. A sample is invalidated if it is corrupted, e.g., by detuned coils during an RF pulse.
- a stream of RF pulse information at the time of the prescription, i.e., before it is played out. The information contains the pulse ID start and end time stamps. By comparing time stamps of RF pulses and PT samples the data streams are synchronized and PT data following a calibration pulse can be identified.
- Valid PT input data is stored in a training buffer BT
- Once 20s of contiguous training data has been collected, calculation of cardiac channel combination data (CCCD) is requested.
- The latest RF pulse preceding the current PT sample is identified.
- RF Calibration training data is identified by RF pulse IDs and stored in a calibration buffer BRF. Once an RF pulse ID indicates the end of the RF Calibration block, calculation of the RF model is requested.
- When CCCD is available, the PT input data is combined into a real valued data stream PTCraw carrying cardiac motion information.
- A Kalman constant velocity filter is applied to the Data to extrapolate the signal during RF pulses, to smoothen it and to calculate its derivative PTCvel in a numerically stable way.
- Trigger are detected on PTCvel
using a threshold-based algorithm. The algorithm also ignores mistriggers
before the last sequence event in a heartbeat (typically a spoiler gradient).
Background thread: calibration calculations
- RF Calibration on buffer BRF:
PT samples are averaged over the pulse train repetitions to suppress physiologic contributions. Invalid samples are removed, and the data is debiased. Then PCA is applied along the time dimension and the first two eigenvectors (corresponding to the two largest eigenvalues) are stored as the RF artefact subspace that should be avoided in coil combinations. Finally, a new calculation of CCCD is triggered. - Calculation of CCCD on buffer
BT:
Training data is debiased and bandpass filtered into two feature data sets for maximum respiratory (0.2Hz to 0.6Hz) and cardiac sensitivity (0.8Hz to 2.5Hz) respectively. The first two eigenvectors of respiratory feature data are selected as respiratory subspace. The part of the first eigenvector of cardiac feature data, that is orthogonal to both the RF artefact subspace and the respiratory subspace, is stored together with the training data mean value as CCCD.
Results
Figure 1 shows the PT signal during RF calibration for different processing stages. RF pulse trains create tiny artefacts with both quickly and slowly decaying components in the raw PT data. However, their amplitude of approximately 1% is substantially larger than the typical cardiac modulation in most channels. Thus, these artefacts distort the output signal PTCvel enough to cause mistriggers. After RF calibration the artefacts are sufficiently suppressed to stabilize trigger detection. Figure 2 demonstrates that the RF suppression is effective for other protocols than the calibration block. Triggering for an inversion time scout protocol (even heart beat: IR-Cine bSSFP 35°, odd heart beat: pause) is unstable before RF calibration and stable after. Figure 3 shows successful triggering for a variety of typical cardiac protocols including GRE and bSSFP readouts in 2D and 3D acquisitions, with multiple preparation schemes including non-selective inversion, saturation, fat saturation, and dark blood preparation.Summary and Outlook
RF interference on Pilot Tone cardiac signals can be effectively suppressed by measuring the RF artefacts in a calibration scan and then avoiding the RF artefact subspace in a PCA based coil combination calculation. This approach has enabled contact-less triggering for complete cardiac examinations. Stability and versatility of the approach warrant further investigations.Acknowledgements
No acknowledgement found.References
- Speier P, Fenchel M, Rehner R: Pt-nav: a novel respiratory navigation method for continuous acquisitions based on modulation of a pilot tone in the MR-receiver. Magn Reson Mater Phys Biol Med 28, 97-98 (2015)
- Schroeder L, Wetzl J, Maier A, Lauer L, Bollenbeck J, Fenchel M, Speier P: A novel method for contact-free cardiac synchronization using the pilot tone navigator. In: Proceedings of the 24th Annual Meeting of ISMRM, Singapore, p. 410 (2016) 3. Vahle T, Bacher M, Rigie D, Fenchel M, Speier P, Bollenbeck J, Schafers KP, Kiefer B, Boada FE: Respiratory motion detection and correction for mr using the pilot tone: Applications for MR and simultaneous PET/MR examinations. Investigative radiology 55(3), 153-159 (2020)
- Vahle T, Bacher M, Rigie D, Fenchel M, Speier P, Bollenbeck J, Schafers KP, Kiefer B, Boada FE: Respiratory motion detection and correction for MR using the pilot tone: Applications for MR and simultaneous PET/MR examinations. Investigative radiology 55(3), 153{159 (2020)
- Bacher M, Speier P, Bollenbeck J, Fenchel M, Stuber M: Pilot tone navigation enables contactless prospective cardiac triggering: initial volunteer results for prospective cine. In: Intl. Soc. Mag. Reson. Med, vol.26, p. 4798 (2018)
- Pruitt A, Liu Y, Jin N, Speier P, Chen C, Simonetti O, and Ahmad R: Evaluating Pilot Tone and self-gating for retrospective cardiac binning in highly accelerated, whole heart 4D flow imaging. In: Proceedings of the 29th Annual Meeting of ISMRM, Online, #2094 (2021)
- Falcão MBL, Di Sopra L, Ma L, Bacher M, Yerly J, Speier P, et al.: Pilot tone navigation for respiratory and cardiac motion-resolved free-running 5D flow MRI. Magn Reson Med. 2021;00:1–15.
- Varghese J, Pan Y, Hayes C, Jin N, Simonetti 0, Speier P: Comparison of Beat Sensor Cardiac Triggering with ECG Triggering in a Comprehensive Cardiac MR Examination: Initial Volunteer Experience. submitted to SCMR 25th Annual Scientific Sessions (2022)
- Hayes C, Huang YT, Kroeker R, Bacher M, Speier P: A complete cardiac MRI examination with pilot tone-based physiological triggering using the BioMatrix Beat Sensor. submitted to SCMR 25th Annual Scientific Sessions (2022)
Figures
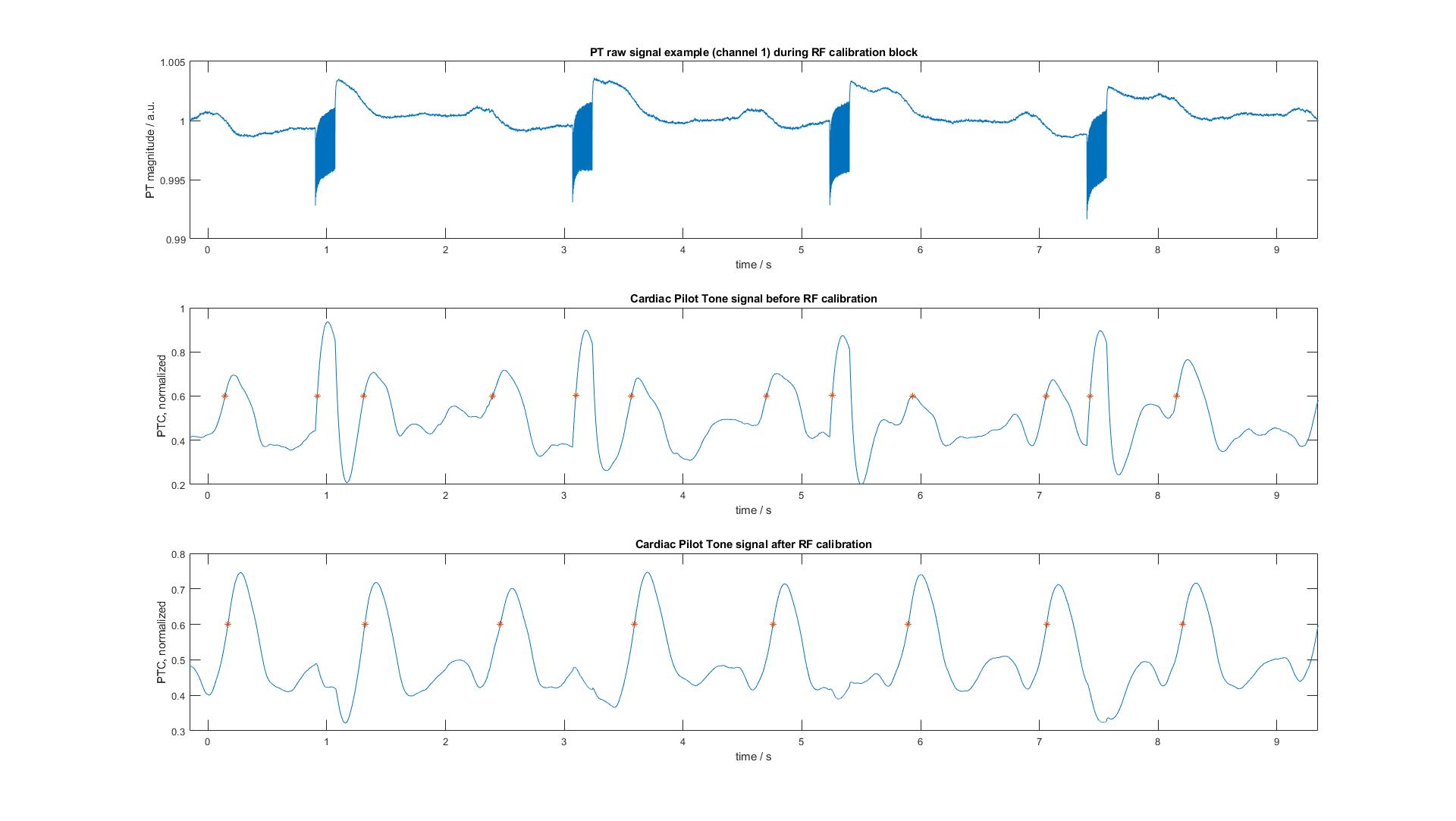
Figure 1. PT
signal during RF calibration block. Top. Magnitude of raw PT signal in an
exemplary receive channel. Middle. PTCvel output signal and detected trigger time points without RF
correction. Bottom. PTCvel output signal and detected trigger time points with RF correction
applied
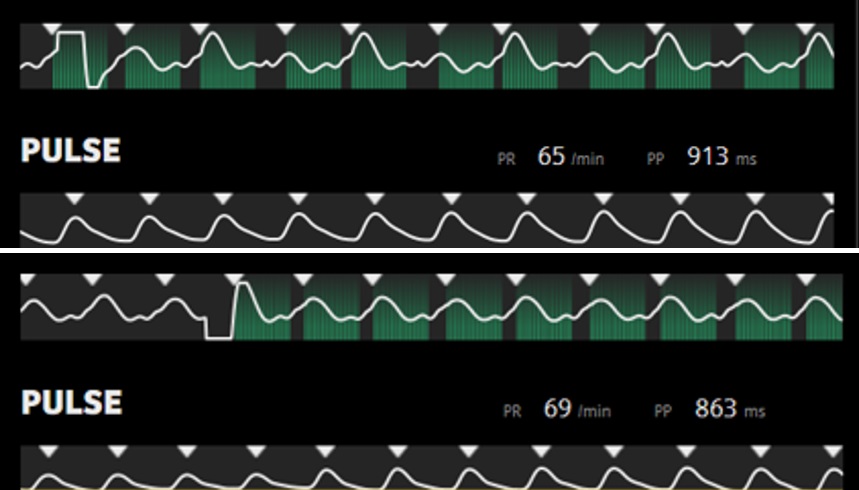
Figure 2. Pilot
Tone cardiac triggering during an exemplary protocol with inhomogeneous RF
(TI-Scout). Shown is PTCvel with triangles indicating the trigger time
points together with a pulse trigger trace for reference. The protocol has an RF periodicity of two
cardiac intervals: even heart beat: IR-Cine bSSFP, flip angle 35°, odd heart beat: pause. Top. Severe artefacts cause mis-triggering before RF calibration. Bottom. Reliable triggering after RF
calibration. The artefact at the start of the measurement results from
activation of the processing prototype.
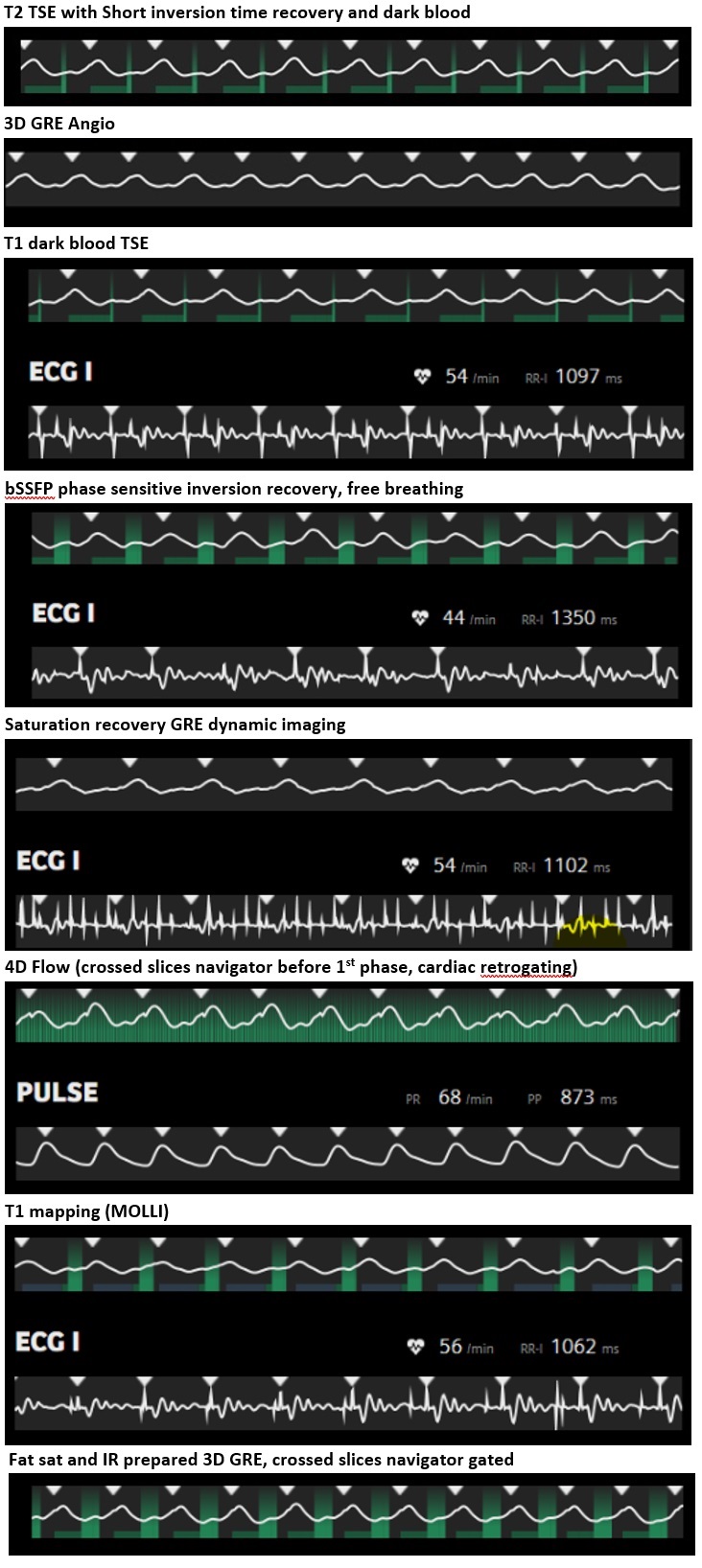
Figure 3. Pilot
Tone Cardiac Triggering for various clinical protocols. For each protocol, PTCvel is shown on top with triangles indicating the trigger time
points, and below, if available, an ECG or pulse oximeter trigger trace for reference. PT trigger time points are delayed by approx. 200ms with respect to the R-wave.
DOI: https://doi.org/10.58530/2022/1653