1623
Head-tilting in diffusion weighted imaging to reduce susceptibility-induced signal dropout in the frontal cortex: feasibility study.1Medical Imaging AI Research Center, Canon Medical Systems Korea, Seoul, Korea, Republic of, 2Department of Radiology, Seoul National University, Seoul, Korea, Republic of, 3Department of Biomedical Engineering, Sungkyunkwan University, Suwon, Korea, Republic of, 4Magnetic Resonance Business Unit, Canon Medical Systems Korea, Seoul, Korea, Republic of
Synopsis
Diffusion-weighted MRI is a highly sensitive to alteration in the movement of water molecules and allows the assessment of various pathologies. Interpretation of the changes can be obscured by signal-dropout due to tissue-air susceptibility difference at the boundaries of nasal cavities, especially in the prefrontal region. The head tilting (chin-up) method during the brain scan could be considered as an accessible way without additional hardware- or sequence to prevent those susceptibility-induced signal-dropout. We demonstrated DWI with head-tilting (up to 20°) resulted in had less severe signal dropout and improved image quality than normal scan in the prefrontal cortex.
Introduction
Diffusion-weighted MRI (DWI) is highly sensitive to alteration in the movement of water molecules and allows the assessment of various pathologies. Interpretation of the changes can be obscured by signal dropout due to tissue-air susceptibility difference at the boundaries of nasal cavities, especially in the prefrontal region. The head tilting (chin-up) method during the brain scan could be considered as an accessible way without additional hardware or sequence to prevent those susceptibility-induced signal-dropout1. As we know, no study has been done previously to investigate the effect of head-tilting method on echo-planar DWI. Therefore, in this study, we aimed to examine DWI scans with the head tilted method compared with a normal position and demonstrate its benefits in signal recovery in the prefrontal region.Methods
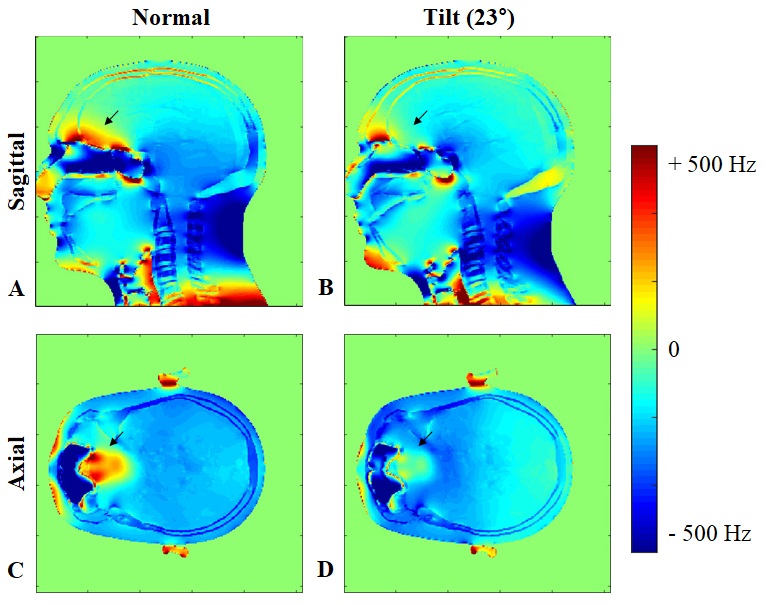
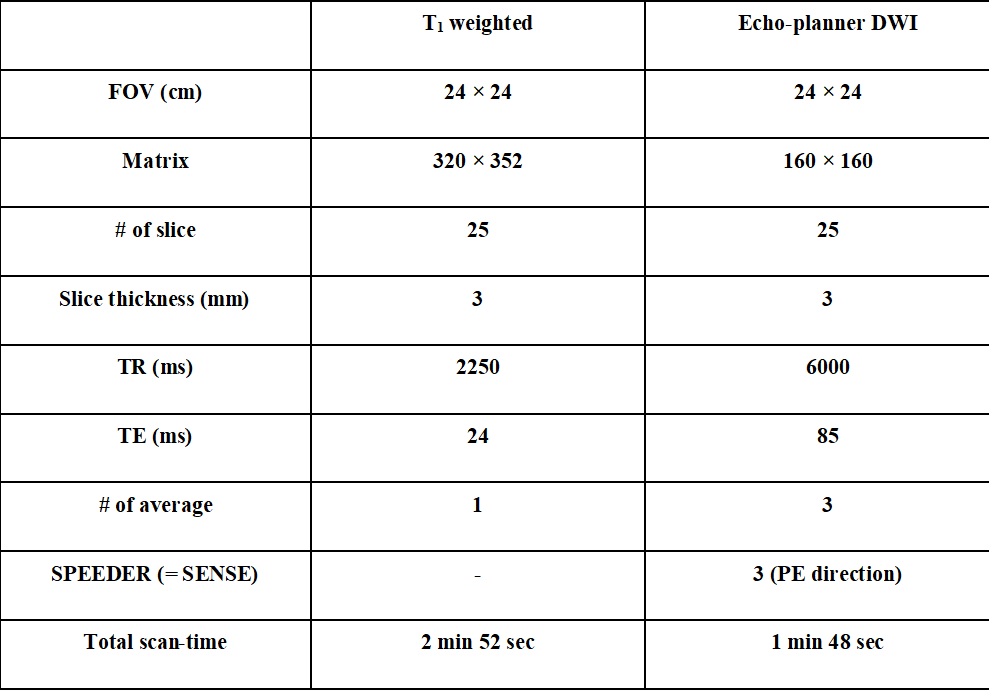
Three healthy subjects (male; 27~35 yo) were scanned on a 3T Vintage Titan (Canon Medical Systems) with a 16-channel head and neck coil using DWI with the same parameters on both normal (approximately parallel to B0) and head tilted (chin-up) methods. For the tilted orientation scan the subject’s torso was elevated about 8 - 10 cm using foam pads under the back, after which the head naturally dropped in the coil housing. This posture resulted in tilt angles with B0 between 20° ~ 25° without excessive neck strain. DWI and T1 weighted images as a reference scan were performed to investigate the signal dropout and recovery in the prefrontal region. Specific scan parameters are listed in Table 1. Simulated B0 maps in a human head model for different orientations are shown in Fig 1. The susceptibility-induced B0 maps for different field directions were calculated with an in-house developed code based on susceptibility voxel convolution1,2. In the tilt model calculation, the applied field direction was changed by rotating it anteriorly in the sagittal plane by a positive angle of 23°. Detailed information on this simulation can be found by Yoo and Lee et al.1,2.Results
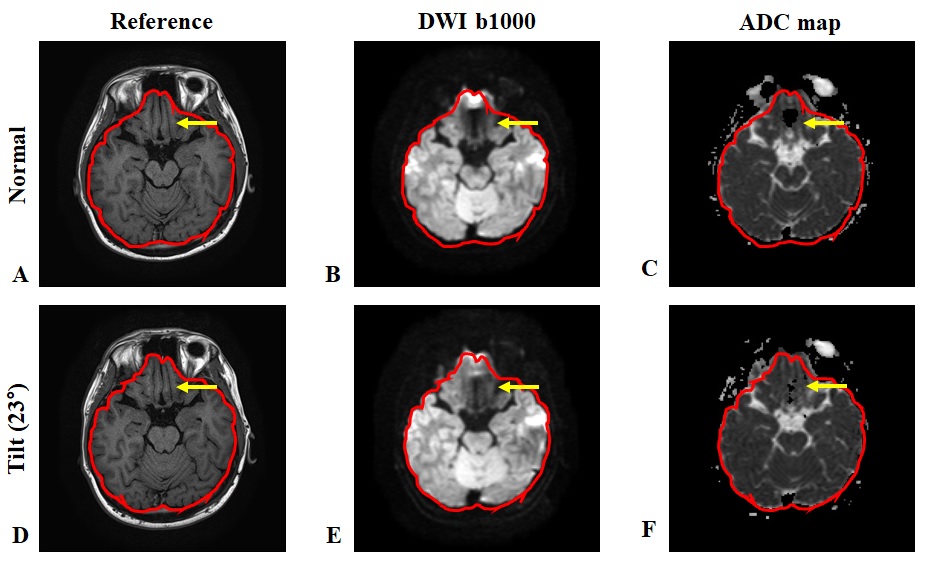
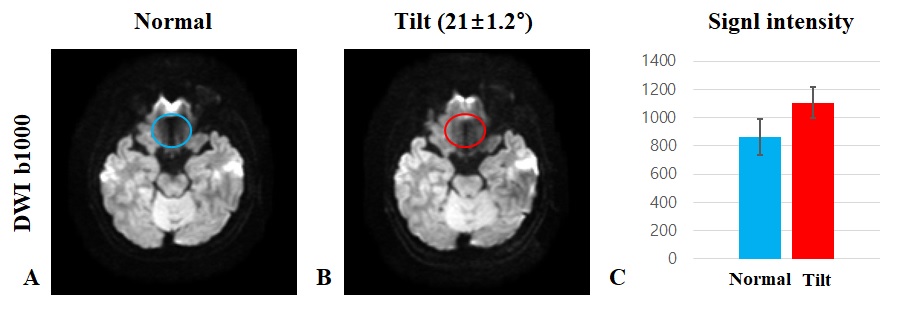
Figure 1 illustrates B0 simulation maps in different field directions at 3T magnetic field ranges. The black arrows indicate B0 inhomogeneity near the prefrontal region. The local field of the prefrontal region was improved with the 23° tilting (B, D) over the normal methods (A, C). Figure 2 shows DWI and ADC maps in normal (A ~ C) and head-tilted scans (D ~ F) with the T1 weighted image as the reference. The head tilted scans resulted in reduced signal-dropout in the prefrontal region compared to normal orientation scans (yellow arrows). Figure 3C shows the mean signal intensities of the same ROI (region of interest) from the prefrontal cortex (A, B) where the less signal dropout was observed in the head tilted scans.Discussion & Conclusion
We demonstrated DWI with head tilting (up to 20°) resulted in less severe signal dropout and improved image quality than normal scan in the prefrontal cortex without additional hardware or pulse sequence. Therefore, recovering the signal loss through this method could improve the evaluation of pathological changes in the frontal cortex. Also, the unconventional scan posture was well tolerated by all the recruited subjects. Further studies are needed to investigate the dependence of tilted angle because, for example, tilted angle degree might affect signal recovery effect as well as bring about neck strain to subject. As reported previously, B0 homogeneity of the prefrontal region is expected to be significantly improved with substantial head tilting (up to 30°) in the chin-up direction1. Moreover, combining coil-based or sequence-based shimming strategies to the head tilt method could improve its effectiveness.Acknowledgements
No acknowledgement found.References
[1] Yoo S et al. Feasibility of head-tilted brain scan to reduce susceptibility-induced signal loss in the prefrontal cortex in gradient echo-based imaging. NeuroImage 2020;223:117265.
[2] Lee S et al. Rapid, theoretically artifact-free calculation of static magnetic field induced by voxelated susceptibility distribution in an arbitrary volume of interest. Magnetic resonance in medicine. 2018;80:2109-2121.
Figures