1616
Spiral UTE MRI of the Lung: An Investigation on Motion Sensitivity1BioMedical Engineering and Imaging Institute, Icahn School of Medicine at Mount Sinai, New York, NY, United States, 2Department of Radiology, Icahn School of Medicine at Mount Sinai, New York, NY, United States, 3MR Application Predevelopment, Siemens Healthcare GmbH, Erlangen, Germany
Synopsis
Spiral UTE is a relatively new MRI technique that combines ultra-short echo time acquisition with a stack-of-spirals trajectory for imaging the lung. In this work, we aimed to analyze the motion sensitivity of different reordering schemes and breath holding positions in spiral UTE MRI to determine the optimized protocol for imaging the lungs. A blind assessment was performed by three experienced chest radiologists and the results were analyzed with statistical tests. The Spiral UTE with line-in-partition reordering performed during the inspiration phase was considered the best protocol in our study.
Introduction
MRI with ultra-short echo time using a stack-of-spirals trajectory (spiral UTE) has been a relatively new method for imaging the lungs without contrast media [1-6]. Compared to more conventional UTE-MRI acquisition based a half-spoke 3D radial trajectory, spiral UTE has increased imaging efficiency that can enable 3D MRI of the lung within a single breath hold. This technique has been demonstrated in several lung MRI studies with encouraging performance [1-6]. Using the stack-of-spirals trajectory, k-space can be acquired with different reordering schemes, as shown in Figure 1. Specifically, stack-of-spirals k-space data can be acquired with either a line-in-partition scheme or a partition-in-line scheme. For the line-in-partition scheme, all spiral interleaves for a given partition are acquired first before moving to the next partition; while for the partition-in-line scheme, all spiral interleaves at a given acquisition angle are acquired before moving to the next acquisition angle. Thus, different reordering schemes can lead to different performance particularly in presence of motion (e.g. cardiac motion or failed breath hold). In this study, we aimed to investigate the performance of spiral UTE-MRI of the lung using both reordering schemes. We also compared images acquired during different breath holding positions.Methods
Spiral UTE-MRI was performed in a total of 31 subjects (15 males, 16 females, mean age= 44.6±14.6 years) using a prototype spiral UTE VIBE sequence. For each subject, four 3D spiral UTE datasets were acquired, including two acquired with the line-in-partition ordering scheme in inspiratory and expiratory breath-hold positions, respectively, and two acquired with the partition-in-line ordering scheme in inspiratory and expiratory breath-hold positions, respectively. Each spiral data was acquired under a single breath hold of ~18 seconds. For comparison, two additional data were also acquired using a 3D breath-hold Cartesian GRE sequence in both inspiratory and expiratory breath-hold positions (see in Figure 2 all protocols acquired).All images were pooled and randomized for blind assessment by three experienced chest radiologists. All readers independently scored the large arteries, large airways, segmental arteries, segmental broncho vascular structures, subsegmental vessels and also the overall artifact level based on a 5-1 scale, where 5 to 1 indicates the best image quality to the worst or the most artifacts to the least. The results were summarized for each assessment category as mean ± standard deviation. The Wilcoxon Signed-Rank test was used to evaluate the difference between different acquisition schemes, with P<0.05 indicating statistical significance.
Results and Discussion
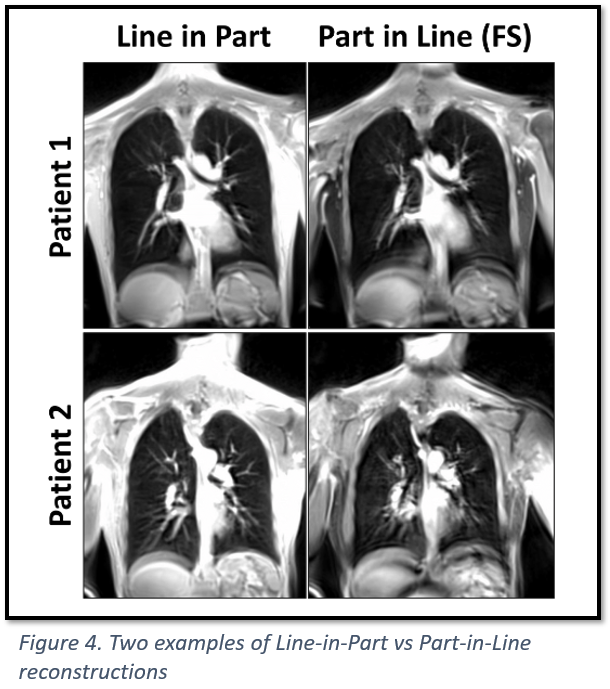
The average scores from different data acquisition schemes are shown in Figure 2. Overall, our results have also shown that spiral UTE images acquired during the inspiratory breath-hold position are significantly better (P<0.05) and can be more robust than the other spiral imaging schemes. This is expected, since it is easier for patients to hold their breath after inhalation, thus reducing the risk of getting motion artifacts. This, in fact, is preferred for lung MRI since more lung space can be visualized when it is expanded, and routine chest CT images are also typically acquired during an inspiratory breath hold position. Spiral UTE with the line-in-partition reordering performed in the inspiratory breath-hold position also received significantly higher scores (P<0.05) than 3D Cartesian images except for the large arteries in the inspiratory breath-hold position (see Figure 2). Figure 3 compares spiral and Cartesian images in a volunteer to demonstrate the improved motion robustness with spiral sampling.Our results have also shown that spiral UTE images acquired with the partition-in-line reordering are more sensitive to motion, as shown in Figure 4. This is because the line-in-partition reordering aims to minimize in-plane motion given the efficient k-space sampling with spiral k-space sampling. On the other side, spiral UTE with the partition-in-line reordering aims to minimize through-plane motion, while motion (such as motion from cardiac beating or failed breath hold) could occur when sampling from one spiral stack to the next. However, it should be noted that when data acquisition is performed during free breathing, the partition-in-line may be better to track motion and sorting the acquired data into different motion phases. Also, the partition-in-line reordering is the scheme to use when fat saturation is needed.
Conclusion
In this study, we investigated the reordering scheme and breath hold position that are preferred when using the spiral UTE sequence. Our results have shown that breath-hold spiral UTE MRI with the line-in-partition scheme is consistently better than the partition-in-line scheme. In addition, we have also shown that images acquired during inspiration are better than that acquired in expiration. We believe these investigations are important to guide users who are interested in using this imaging technique and for better translation of this new method into the clinic.Acknowledgements
This project was supported in part by NIH R01EB031083.References
[1] John P. Mugler, Samuel W. Fielden, Craig H. Meyer, Talissa A. Altes, G. Wilson Miller, Alto Stemmer, Josef Pfeuffer, and Berthold Kiefer “Breath-hold UTE Lung Imaging using a Stack-of-Spirals Acquisition”. ISMRM 2015, p 1476
[2] John P. Mugler, Craig H Meyer, Josef Pfeuffer, Alto Stemmer, and Berthold Kiefer. “Accelerated Stack-of-Spirals Breath-hold UTE Lung Imaging”. ISMRM 2017, p 4904
[3] Heidenreich JF, Weng AM, Metz C, Benkert T, Pfeuffer J, Hebestreit H, Bley TA, Köstler H, Veldhoen S. “Three-dimensional Ultrashort Echo Time MRI for Functional Lung Imaging in Cystic Fibrosis” Radiology. 2020 Jul;296(1):191-199
[4] Corona Metz, David Böckle, Julius Frederik Heidenreich, Andreas Max Weng, Thomas Benkert, Götz Ulrich Grigoleit, Thorsten Bley, Herbert Köstler, Simon Veldhoen. “Pulmonary Imaging of Immunocompromised Patients during Hematopoietic Stem Cell Transplantation using Non-Contrast-Enhanced Three-Dimensional Ultrashort Echo Time (3D-UTE) MRI” Rofo . 2021 Oct 14. doi: 10.1055/a-1535-2341
[5] Daniel Gräfe, Rebecca Anders, Freerk Prenzel, Ina Sorge, Christian Roth, Thomas Benkert, Franz Wolfgang Hirsch. “Pediatric MR lung imaging with 3D ultrashort-TE in free breathing: Are we past the conventional T2 sequence?” Pediatr Pulmonol . 2021 Sep 7. doi: 10.1002/ppul.25664
[6] Simon Veldhoen, Julius F Heidenreich, Corona Metz, Bernhard Petritsch, Thomas Benkert, Helge U Hebestreit, Thorsten A Bley, Herbert Köstler, Andreas M Weng “Three-dimensional Ultrashort Echotime Magnetic Resonance Imaging for Combined Morphologic and Ventilation Imaging in Pediatric Patients With Pulmonary Disease” J Thorac Imaging . 2021 Jan;36(1):43-51
Figures
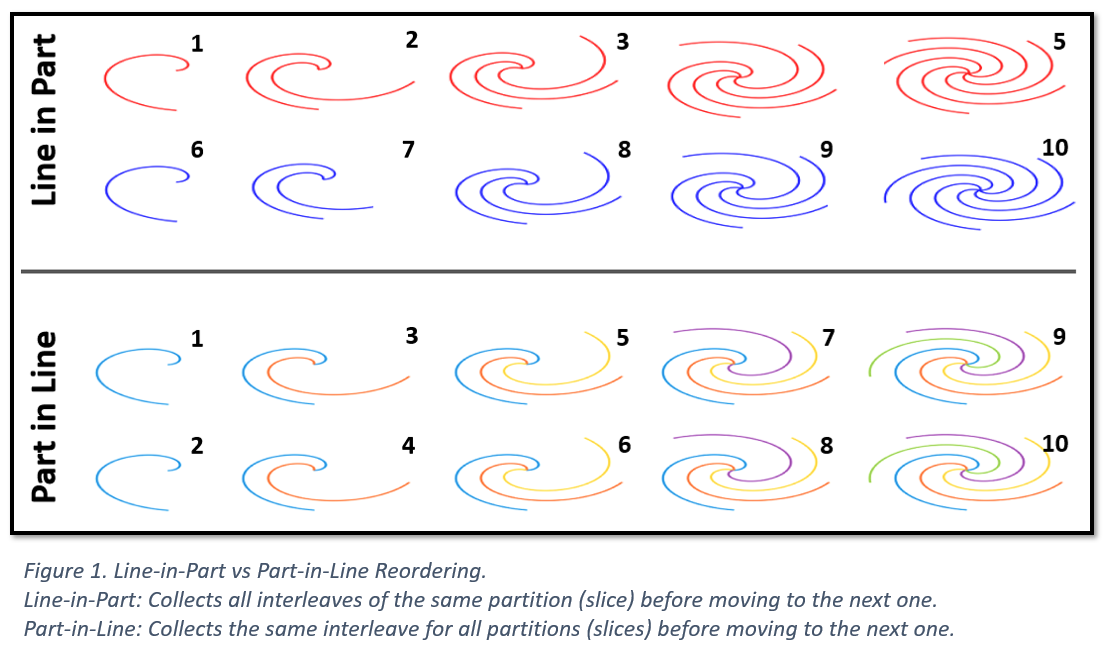
Figure 1. Line-in-Part vs Part-in-Line Reordering.
Line-in-Part: Collects all interleaves of the same partition (slice) before moving to the next one.
Part-in-Line: Collects the same interleave for all partitions (slices) before moving to the next one.
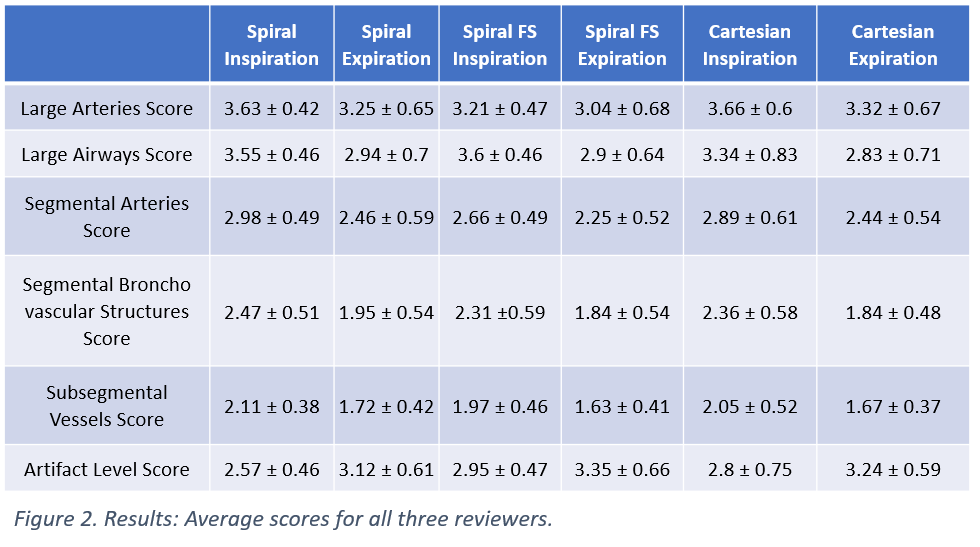
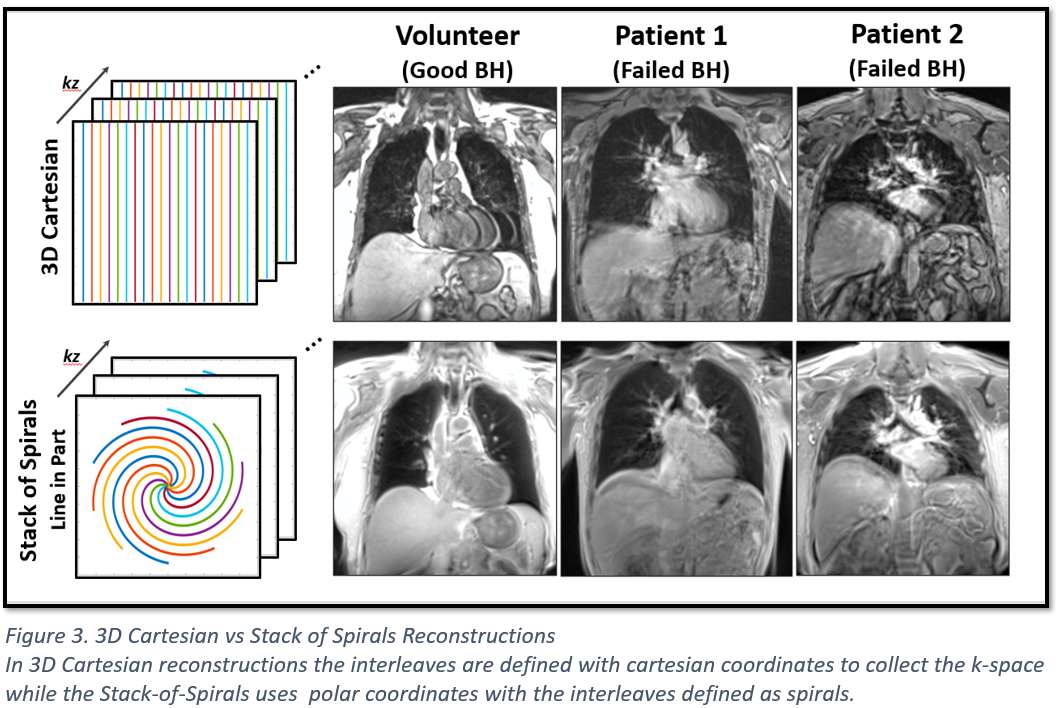
Figure 3. 3D Cartesian vs Stack of Spirals Reconstructions
In 3D Cartesian reconstructions the interleaves are defined with cartesian coordinates to collect the k-space while the Stack-of-Spirals uses polar coordinates with the interleaves defined as spirals.