1583
Combining DCE and DSC-MRI in Arterial Input Function Estimation Using Multi-Channel Blind Deconvolution1Institute of Scientific Instruments of the Czech Academy of Sciences, Brno, Czech Republic, 2Central European Institute of Technology, Masaryk University, Brno, Czech Republic
Synopsis
We propose to combine DCE and DSC-MRI in a simultaneous acquisition and processing scheme to provide more information for estimation of the arterial input function using multi-channel blind deconvolution. On simulated and flow-phantom data, we show that DCE-DSC blind deconvolution is superior to standard DCE blind deconvolution, especially for low signal-to-noise-ratio conditions.
Introduction
Lack of reliable methods for estimation of the arterial input function (AIF) is one of the main problems in DCE-MRI. Blind deconvolution1 is a method, where the AIF is estimated from selected tissue curves (channels) by fitting them with a convolutional pharmacokinetic model where the AIF is one term of the convolution. It avoids the problems of AIFs measured in large arteries (flow, partial-volume, saturation, dispersion artifacts) or population-based AIFs (ignoring subject-specific AIF variations). However, blind deconvolution is often an ill-posed or even non-unique inversion problem and additional information is needed to overcome it.Methods
We propose a novel blind-deconvolution approach combining DCE and DSC signals. For this purpose, we have implemented simultaneous compressed-sensing DCE-DSC acquisition, using Multi-Echo Golden-Angle Stack-Of-Stars (MEGA-SOS), followed by total-variance image-sequence reconstruction2, separately for each slice and echo time, and fitting of the T2*-relaxation model to each voxel at each time instant3, leading to DCE and DSC tissue curves estimated for each voxel.The mean DCE and DSC curves within the selected regions (channels) are then simultaneously fitted with the GCM model3, linking the DCE and DSC signals together, giving the estimated AIF (and perfusion parameters of the selected regions).
The methodology was validated on synthetic data (6 channels with randomly generated perfusion parameters, mice AIF model4, ATH pharmacokinetic model, 50 noise realizations per SNR). Dynamic-phantom data were measured with a 3T Siemens Prisma scanner with own implementation of the MEGA-SOS method (6 echoes with TE=2.5;5.2;7.9;10.6;13.3;16ms, TR=20ms, FA=30deg, 12 slices, FOV 150x150mm). An open-loop circuit with a dialyzer filter and a peristaltic pump (250 mL/min) was used. Contrast-agent boli were administered manually in the doses of 0.5 and 1.0 mL of 1:9 dilution of MultiHance (Bracco Imaging, Italy).
Results
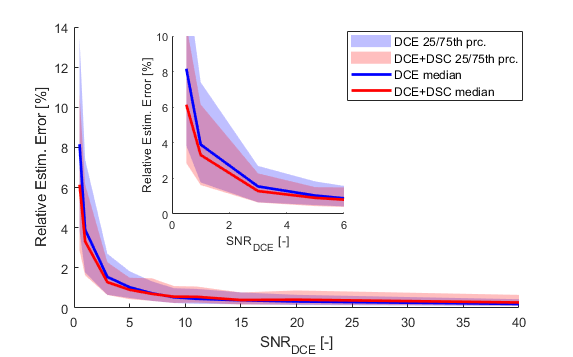
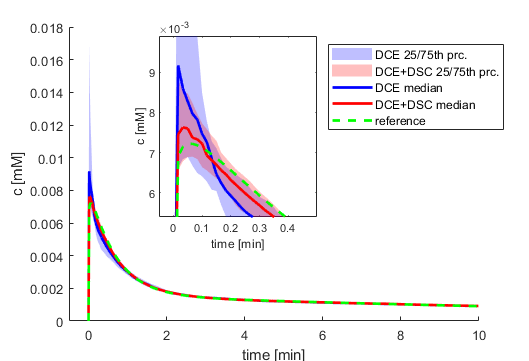
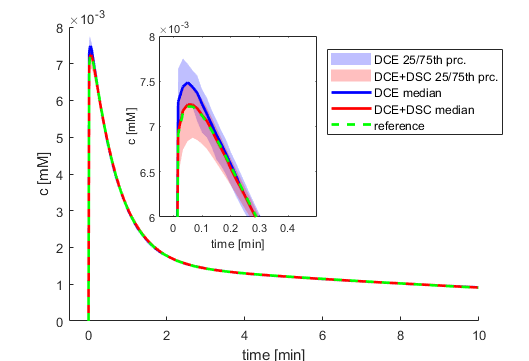
DCE-DSC blind deconvolution outperformed the standard DCE version under low-SNR conditions up to SNR=6, concerning both the median error and the width of its confidence intervals (Fig.1), see also an example for SNR=1 and 5 (Figs.2,3).In the phantom experiment, 6 regions of defined lengths were drawn in the middle slice, starting at the proximal edge of the dialyzer (Fig.4) and processed with the DCE and DCE-DSC deconvolution methods (non-parametric AIF assumed). The accuracy was evaluated indirectly based on mean transit times, Tc, estimated for the regions, see description of Fig.5. While the DCE-DSC estimates of Tc were overlapping, the DCE estimates were not consistent.Discussion and conclusion
Blind deconvolution using DCE-DSC leads to more accurate and more precise AIF estimation for low SNR under simulated conditions. The flow phantom results were also more consistent for the proposed DCE-DSC method. In the next step, the potential of the DCE-DSC blind deconvolution will be evaluated on real clinical and preclinical data.Acknowledgements
MEYS, LM2018129 - National Infrastructure for Biological and Medical Imaging.
References
1 Fluckiger M.C. et.al. Model-based blind estimation of kinetic parameters in dynamic contrast-enhanced (DCE)-MRI, MRM-62(2009)1477–1486.
2 Tian, K.C. et.al., Technical Note: Evaluation of pre-reconstruction interpolation methods for iterative reconstruction of radial k -space data, Med.Phys-44(2017) 4025–4034
3 Sourbron S.T2*-relaxivity contrast imaging: First results, MRM-69(2013)1430-1437
4 Jirik R et.al, Blind deconvolution estimation of an arterial input function for small animal DCE-MRI. MagResonImaging62(2019)46-56.
Figures
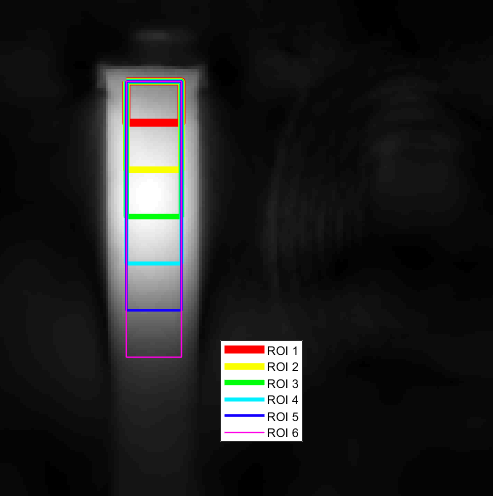
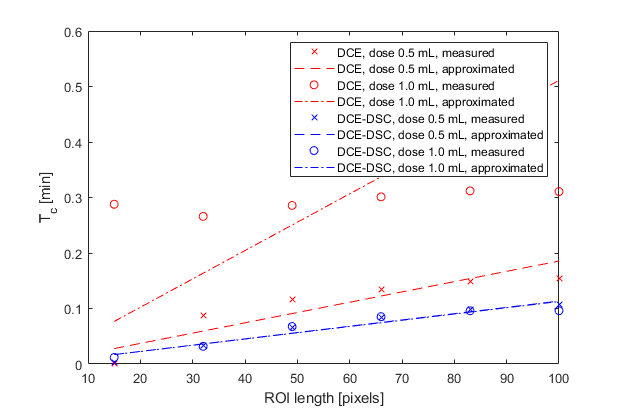
Tc is assumed proportional to the length of the region. The quality of a linear fit to the Tc estimates reflects the accuracy of the blind-deconvolution algorithm.
Better consistency in Tc estimates shows the proposed DCE+DSC method where linear fits overlap.