1567
5D Free-Running-LIBRE MRI for 3D whole-heart Cine: A pilot study in patients at 3T1Radiology, McGill University Health Centre (MUHC), Montreal, QC, Canada, 2Circle Cardiovascular Imaging Inc., Calgary, AB, Canada, 3Diagnostic and Interventional Radiology, Le Centre Hospitalier Universitaire Vaudois (CHUV), Lausanne, Switzerland, 4Center for BioMedical Imaging (CIBM), Lausanne, Switzerland, 5Advanced Clinical Imaging Technology, Siemens Healthcare AG, Lausanne, Switzerland, 6Radiology, Université de Montréal, Montreal, QC, Canada, 7Cardiac Sciences, University of Calgary, Calgary, AB, Canada, 8Heidelberg University, Heidelberg, Germany, 9Diagnostic, Interventional and Pediatric Radiology (DIPR), Inselspital, Bern University Hospital, Bern, Switzerland, 10Translational Imaging Cente, Bern, Switzerland
Synopsis
Cardiac magnetic resonance imaging is often limited by long scan times and the need for multiple breath holds. A Free-Running sequence may overcome this limitation by providing 3-D cine data in a free-breathing non-ECG-triggered acquisition of 7 minutes. The clinical applicability of this method was tested in a cohort of 9 patients with varying pathologies. Myocardial blood-pool volumes and ejection fractions were compared between standard 2-D protocols and 5-D Free-Running-LIBRE. Free-Running-LIBRE successfully quantified volumes and ejection fractions with results correlating strongly to reference measurements. The method demonstrated additional potential to visualize irreversible myocardial injury in these patients.
Background
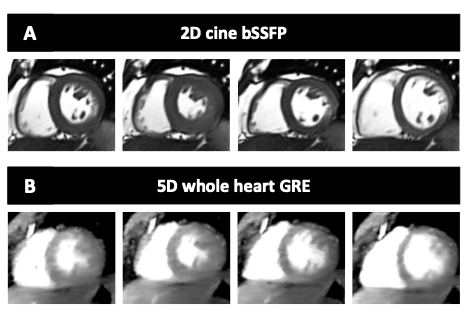
Cardiac magnetic resonance imaging (CMR) is the gold standard assessment for ventricular function but is limited by long scan times and the need for multiple breath holds1,2. A new Free-Running MR imaging sequence3,4,5, integrated with LIBRE water excitation6,7—(Free-Running-LIBRE), may overcome this limitation by providing isotropic, fat-suppressed, 3-D cine data in a single free-breathing non-ECG-triggered acquisition of 7 minutes. Cardiac images can be reconstructed in any plane and cardiac phase to assess morphology and function. The aim of the study was to compare myocardial volumes and ejection fraction (EF) as measured by whole-heart Free-Running-LIBRE compared to standard 2D clinical protocols in patients with mixed pathologies.Methods
Patients referred for a clinically indicated CMR exam were recruited. Exams were conducted on a 3T MRI system (MAGNETOM Skyra™, Siemens Healthcare, Erlangen, Germany). 2D balanced Steady-State Free Precession (bSSFP) images were acquired in 2-chamber (2CH), 3-chamber (3CH), 4-chamber (4CH) views, and as a short axis stack through both ventricles (SAX). Prototype free-Running-LIBRE gradient echo (GRE) data were acquired immediately after the injection of Gadovist™. Seven minutes after injection, late gadolinium enhancement (LGE) images were acquired in 2CH, 3CH, 4CH, and SAX views at end-diastole. Free-Running-LIBRE images were reconstructed using a compressed sensing framework5 and data were used to calculate 2CH, 4CH, 3CH and SAX views using clinically certified software (cvi42, Circle Cardiovascular Imaging Inc., Calgary, AB, Calgary). EF was calculated from SAX stack images. Regression and Bland-Altman analyses were used to compare measurements.Results
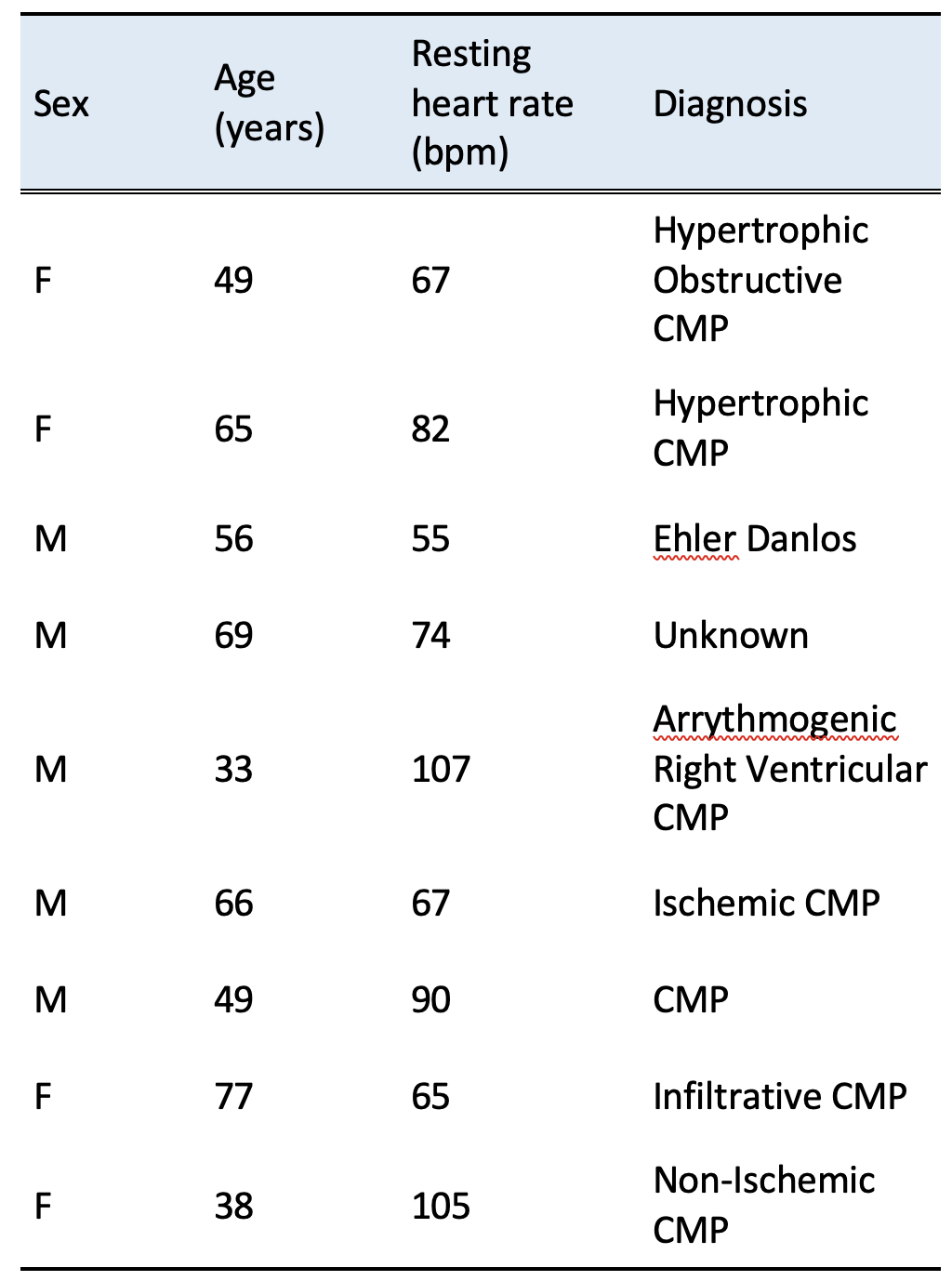
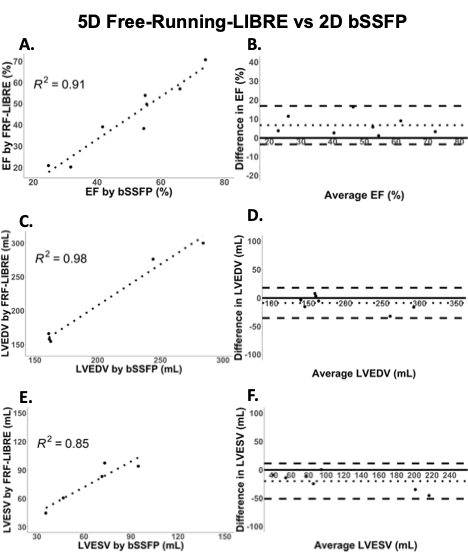
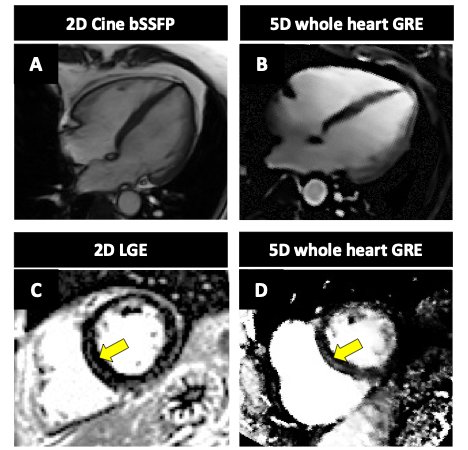
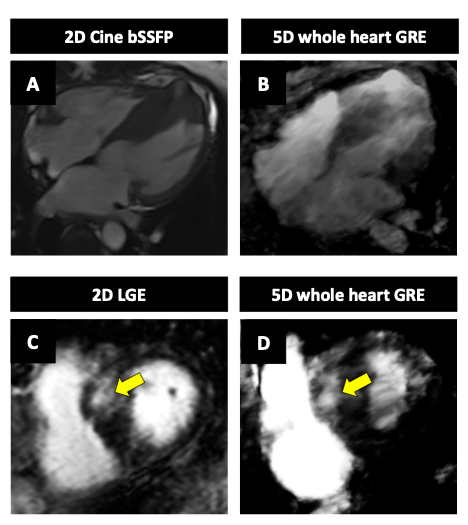
Nine patients with varying pathologies (table 1) were recruited into this study (mean age 56.5y.). Two patients were excluded from analysis due to poor image quality. In the remaining patients, Free-Running-LIBRE results underestimated ejection fraction with an average difference of 5% (Fig. 1A), overestimated end-diastolic volume with an average difference of 8.6 mL (Fig. 1C), and overestimated end-systolic volume with an average difference of 19.8 mL (Fig. 1E). All measurements showed a strong correlation (r2 > 0.85) between methods (Fig. 1B, 1D, 1F). Mid-myocardial enhancement was clearly observed in the same location as LGE images in a patient with Duchenne muscular dystrophy (Fig. 2C and 2D) and in a patient with hypertrophic cardiomyopathy (Fig. 3C and 3D).Conclusion
Our pilot study shows the potential of Free-Running-LIBRE, with a total scan time of 7 minutes, to quantitatively assess myocardial volumes and EF in various clinical pathologies at 3T. It is hypothesized that regularization in the temporal dimensions of the Free-Running MRI reconstruction framework leads to the observed difference seen between quantitative measurements. This hypothesis is currently being investigated. Although further adjustments are required to enhance image quality, this acquisition strategy may have clinical value in patients with trouble holding their breath or in pediatric populations. Furthermore, its potential for visualizing irreversible myocardial injury (LGE) should be further explored.Acknowledgements
No acknowledgement found.References
1 Roifman I, Paterson DI, Jimenez-Juan L, Friedrich MG, Howarth AG, Wintersperger BJ, Thavendiranathan P, White JA, Connelly KA. The State of Cardiovascular Magnetic Resonance Imaging in Canada: Results from the CanSCMR Pan-Canadian Survey. Canadian Journal of Cardiology. 2018 Mar 1;34(3):333-6.
2 Ginat DT, Fong MW, Tuttle DJ, Hobbs SK, Vyas RC. Cardiac imaging: Part 1, MR pulse sequences, imaging planes, and basic anatomy. American Journal of Roentgenology. 2011 Oct;197(4):808-15.
3 Coppo S, Piccini D, Bonanno G, Chaptinel J, Vincenti G, Feliciano H, Van Heeswijk RB, Schwitter J, Stuber M. Free‐running 4D whole‐heart self‐navigated golden angle MRI: initial results. Magnetic resonance in medicine. 2015 Nov;74(5):1306-16.
4 Feng L, Coppo S, Piccini D, Yerly J, Lim RP, Masci PG, Stuber M, Sodickson DK, Otazo R. 5D whole‐heart sparse MRI. Magnetic resonance in medicine. 2018 Feb;79(2):826-38.
5 Di Sopra L, Piccini D, Coppo S, Stuber M, Yerly J. An automated approach to fully self-gated free-running cardiac and respiratory motion-resolved 5D whole-heart MRI. Magn Reson Med. 2019;82(6):2118-2132.
6 Bastiaansen JA, Stuber M. Flexible water excitation for fat‐free MRI at 3T using lipid insensitive binomial off‐resonant RF excitation (LIBRE) pulses. Magnetic resonance in medicine. 2018 Jun;79(6):3007-17.
7 Bastiaansen JA, van Heeswijk RB, Stuber M, Piccini D. Noncontrast free-breathing respiratory self-navigated coronary artery cardiovascular magnetic resonance angiography at 3 T using lipid insensitive binomial off-resonant excitation (LIBRE). Journal of Cardiovascular Magnetic Resonance. 2019 Dec;21(1):1-1.
Figures