1475
TNM and VALSG Stage Assessments in SCLC: Diagnostic Capability Comparison among PET/MRI, PET/CT, Whole-Body MRI and Conventional Examination1Radiology, Fujita Health University School of Medicine, Toyoake, Japan, 2Joint Research Laboratory of Advanced Medical Imaging, Fujita Health University School of Medicine, Toyoake, Japan, 3Canon Medical Systems Corporation, Otawara, Japan, 4Diagnostic Radiology, Hyogo Cancer Center, Akashi, Japan, 5Radiology, Fujita Health University Hospital, Toyoake, Japan
Synopsis
Whole-body MRI and co-registered or integrated PET combined with MRI (PET/MRI) using 1.5 T or 3T MR systems has been suggested as equal to or more accurate than PET/CT or conventional staging or recurrence surveillance methods in thoracic oncologic patients. We hypothesize that whole-body MRI and co-registered PET/MRI for SCLC patients have equal to or superior potential for VALSG and TNM stage assessments than PET/CT and conventional staging method. The purpose of this study was to prospectively compare the capabilities for assessing VALSG and TNM stages among whole-body MRI, PET/MRI, PET/CT and conventional staging method in SCLC patients.
Introduction
Lung cancer is the leading cause of cancer-related death worldwide, and small-cell lung cancer (SCLC) is more aggressive and has a worse prognosis than any other type of lung cancer1. The first SCLC staging system was introduced by the Veterans Administration Lung Cancer Study Group (VALSG) in 1973, and it divided patients into those with ‘limited stage’ (LS) disease, confined to the hemithorax, and those with ‘extensive stage’ (ES) disease at sites beyond those included in LS disease2. The VALSG system was developed at a time when the utility of surgery was being questioned. On the other hand, the tumor, node and metastasis (TNM) staging system has not been considered as applicable to SCLC. However, a few investigators showed that the TNM system was useful for predicting SCLC outcomes3. Surgery and stereotactic body radiotherapy (SBRT) have been suggested as treatments for stage I patients, while combined chemoradiotherapy or chemotherapy has been recommended for other stages. Therefore, accurate clinical stage classification is important for management of SCLC patients in routine clinical practice. In routine clinical practice, conventional staging method are usually used for staging. As an alternative to conventional staging method, however, positron emission tomography (PET) and PET fused with CT (PET/CT) combined with [18F] fluoro-2-D-glucose (FDG) has been suggested as useful in this setting. Moreover, whole-body MRI and co-registered or integrated PET combined with MRI (PET/MRI) using 1.5 tesla (T) or 3T MR systems has been suggested as equal to or more accurate than PET/CT or conventional staging or recurrence surveillance methods in not only NSCLC, but also other thoracic oncologic patients4-7. We hypothesize that whole-body MRI and co-registered PET/MRI for SCLC patients have equal to or superior potential for VALSG and TNM stage assessments than PET/CT and conventional staging method. The purpose of this study was to prospectively compare the capabilities for assessing VALSG and TNM stages among whole-body MRI, PET/MRI, PET/CT and conventional staging method in SCLC patients.Materials and Methods
Ninety-eight patients (71.7±7.8 years, range: 40-83 years) including 64 males (70.7±7.8 years; age range, 54-80 years) and 34 females (73.6±7.3 years; age range, 47-83 years)underwent whole-body MRI at three 3T MR systems (Vantage Titan 3T, Vantage Galan 3T [ym正C○1] and Vantage Centurian, Canon Medical Systems Corporation, Otawara, Japan), FDG-PET/CT and conventional staging method before treatment. Standard references for each factor, TNM stage and VALSG stages were determined by tumor board consisted with diagnostic radiologists, pulmonary physicians, radiation oncologists and pathologists, whose experiences were more than 10 years experiences. Then, T, N and M factors, TNM and VALSG stages were independently evaluated by two investigators, and final diagnoses were made by consensus of two investigators. Firstly, weighted kappa statistics were performed to determine interobserver agreements of all factors and both clinical stage classifications between two investigators. Secondly, agreements of all factors as well as each clinical stage between final diagnosis and each method evaluation were determined by weighted kappa statistics. Finally, diagnostic accuracy of each factor, TNM and VALSG stage evaluations were statistically compared among all methods by using McNemar’s test. A p value less than 0.05 was considered as significant at each statistical analysis.Results
Representative case is shown in Figure 1 and 2. Interobserver agreements for T, N and M factors, TNM stage and VALSG stage assessments on all methods are shown in Figure 3. All interobserver agreements on each method were determined as significant and almost perfect (0.81≤κ, p<0.0001). When assessed agreements and diagnostic accuracy for T factor between final diagnosis and each method, agreement of each method was significant and almost perfect (0.86≤κ, p<0.0001). In addition, accuracies of whole-body MRI and PET/MRI were significantly higher than that of PET/CT (p<0.05). When assessed agreements and diagnostic accuracy for N factor between final diagnosis and each method, agreement of each method was significant and substantial (0.67≤κ≤0.80, p<0.0001). Moreover, accuracies of whole-body MRI, PET/MRI and PET/CT were significantly higher than that of conventional staging method (p<0.05). When assessed agreements and diagnostic accuracy for M factor between final diagnosis and each method, agreement of each method was significant and substantial or almost perfect (0.67≤κ, p<0.0001). In addition, accuracies of whole-body MRI, PET/MRI and PET/CT were significantly higher than that of conventional staging method (p<0.05). Agreements and diagnostic accuracy for TNM staging between final diagnosis and each method are shown in Figure 4. Agreement of each method was significant and substantial or almost perfect (0.68≤κ, p<0.0001). Moreover, accuracies of whole-body MRI and PET/MRI were significantly higher than that of PET/CT and conventional staging method (p<0.05). Agreements and diagnostic accuracy for VALSG staging between final diagnosis and each method are shown in Figure 5. Agreement of each method was significant and almost perfect (0.83≤κ, p<0.0001). Moreover, accuracies of whole-body MRI and PET/MRI were significantly higher than that of PET/CT and conventional staging method (p<0.05).Conclusion
Whole-body MRI and PET/MRI have equal to or higher capabilities for T, N and M factor assessments and TNM and VALSG stage evaluations, when compared with PET/CT or conventional staging method.Acknowledgements
This study was technically and financially supported by Canon Medical Systems Corporation.References
- van Meerbeeck JP, Fennell DA, De Ruysscher DK. Small-cell lung cancer. Lancet. 2011;378(9804):1741-1755.
- Zelen M. Keynote address on biostatistics and data retrieval. Cancer Chemother Rep 3. 1973;4(2):31-42.
- Nicholson AG, Chansky K, Crowley J, et al; Staging and Prognostic Factors Committee, Advisory Boards, and Participating Institutions; Staging and Prognostic Factors Committee Advisory Boards and Participating Institutions. The International Association for the Study of Lung Cancer Lung Cancer Staging Project: Proposals for the Revision of the Clinical and Pathologic Staging of Small Cell Lung Cancer in the Forthcoming Eighth Edition of the TNM Classification for Lung Cancer. J Thorac Oncol. 2016;11(3):300-311.
- Ohno Y, Koyama H, Yoshikawa T, et al. Three-way Comparison of Whole-Body MR, Coregistered Whole-Body FDG PET/MR, and Integrated Whole-Body FDG PET/CT Imaging: TNM and Stage Assessment Capability for Non-Small Cell Lung Cancer Patients. Radiology. 2015;275(3):849-861.
- Ohno Y, Kishida Y, Seki S, et al. Comparison of Interobserver Agreement and Diagnostic Accuracy for IASLC/ITMIG Thymic Epithelial Tumor Staging Among Co-registered FDG-PET/MRI, Whole-body MRI, Integrated FDG-PET/CT, and Conventional Imaging Examination with and without Contrast Media Administrations. Acad Radiol. 2018:S1076-6332(17)30542-1.
- Ohno Y, Yui M, Aoyagi K, Kishida Y, Seki S, Koyama H, Yoshikawa T. Whole-Body MRI: Comparison of Its Capability for TNM Staging of Malignant Pleural Mesothelioma With That of Coregistered PET/MRI, Integrated FDG PET/CT, and Conventional Imaging. AJR Am J Roentgenol. 2019;212(2):311-319.
- Ohno Y, Takeshi Y, Takenaka D, Koyama H, Aoyagi K, Yui M. Comparison of Diagnostic Accuracy for TNM Stage Among Whole-Body MRI and Coregistered PET/MRI Using 1.5-T and 3-T MRI Systems and Integrated PET/CT for Non-Small Cell Lung Cancer. AJR Am J Roentgenol. 2020;215(5):1191-1198.
Figures
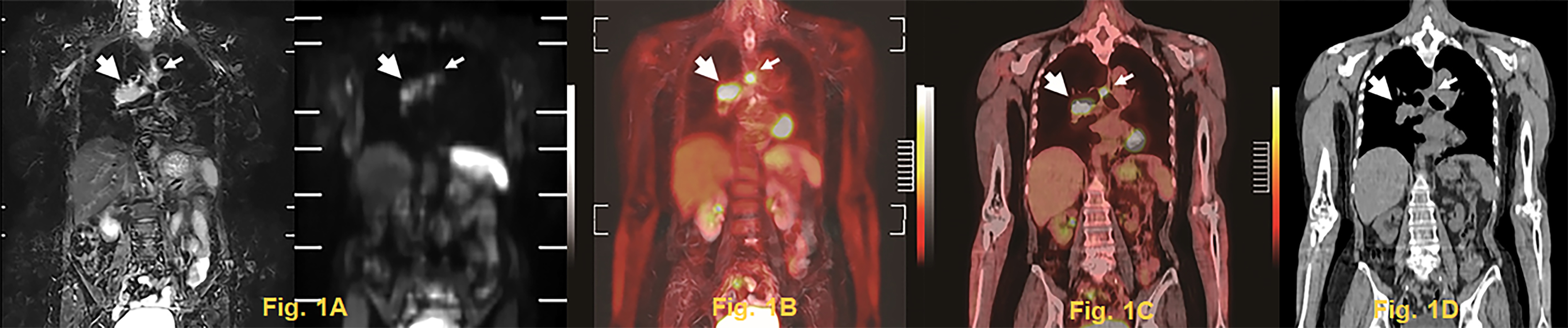
Figure 1. 68-year-old pathologically diagnosed small cell carcinoma patient with asthma.
Whole-body MRI (Fig. 1A: L to R, STIR image and DWI), PET/MRI (Fig. 1B) , PET/CT (Fig. 1C) and multiplanar reconstructed image from unenhanced CT (Fig. 1D) show primary lesion in the right hilum (large arrow) and mediastinal lymph node metastasis (small arrow). MRI, PET/MRI and PET/CT accurately diagnosed this case. Unenhanced CT accurately diagnosed N and M factors and each stage in this case.
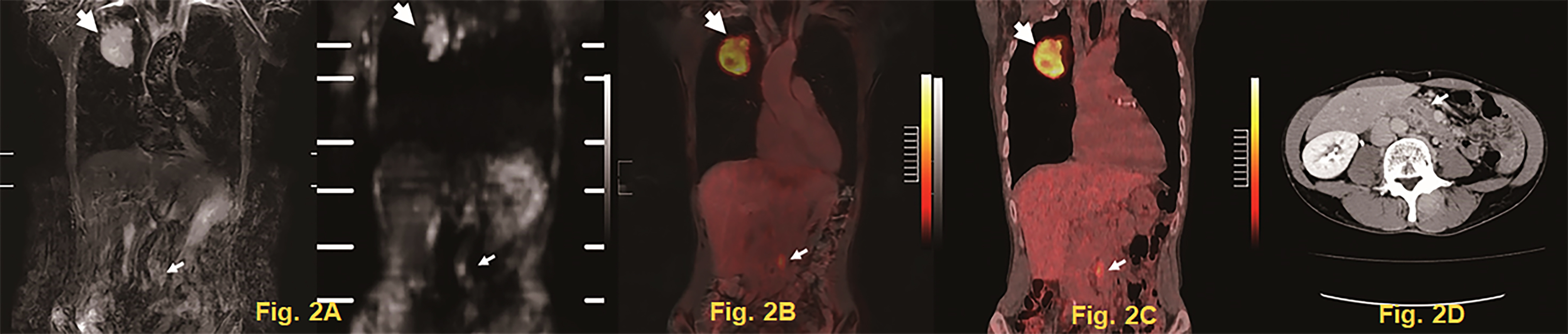
Figure 2. 57-year-old pathologically diagnosed small cell carcinoma patient.
Whole-body MRI (Fig. 2A: L to R, STIR image and DWI), PET/MRI (Fig. 2B) and PET/CT (Fig. 2C) demonstrate primary lesion in the right upper lobe (large arrow) on STIR image and DWI and abdominal lymph node metastasis (small arrow). Contrast-enhanced CT on axial plane (Fig. 2D) was missed abdominal lymph node metastasis (small arrow) in this case.
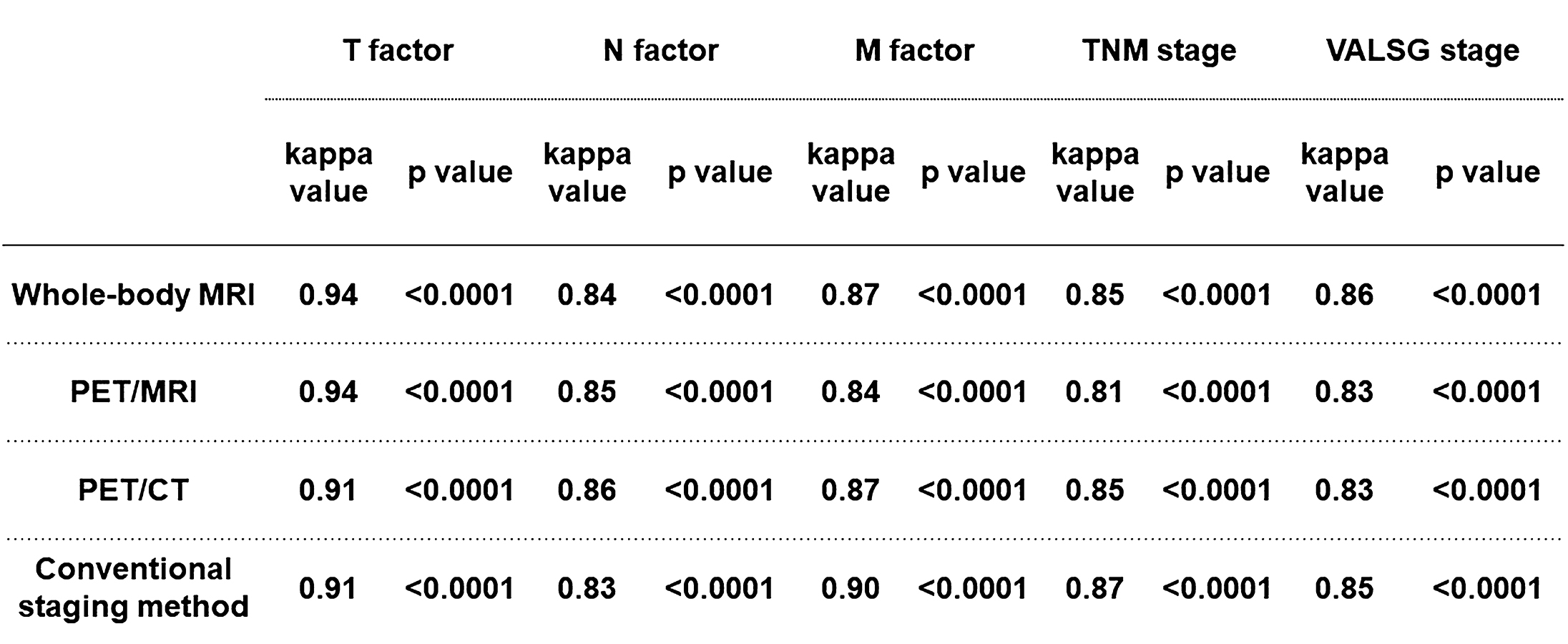
Figure 3. Inter-observer agreements for T, N and M factors, TNM stage and VALSG stage assessments on whole-body MRI, PET/MRI, PET/CT and conventional staging method.
Each interobserver agreement was evaluated as significant and almost perfect (0.81≤κ, p<0.0001).
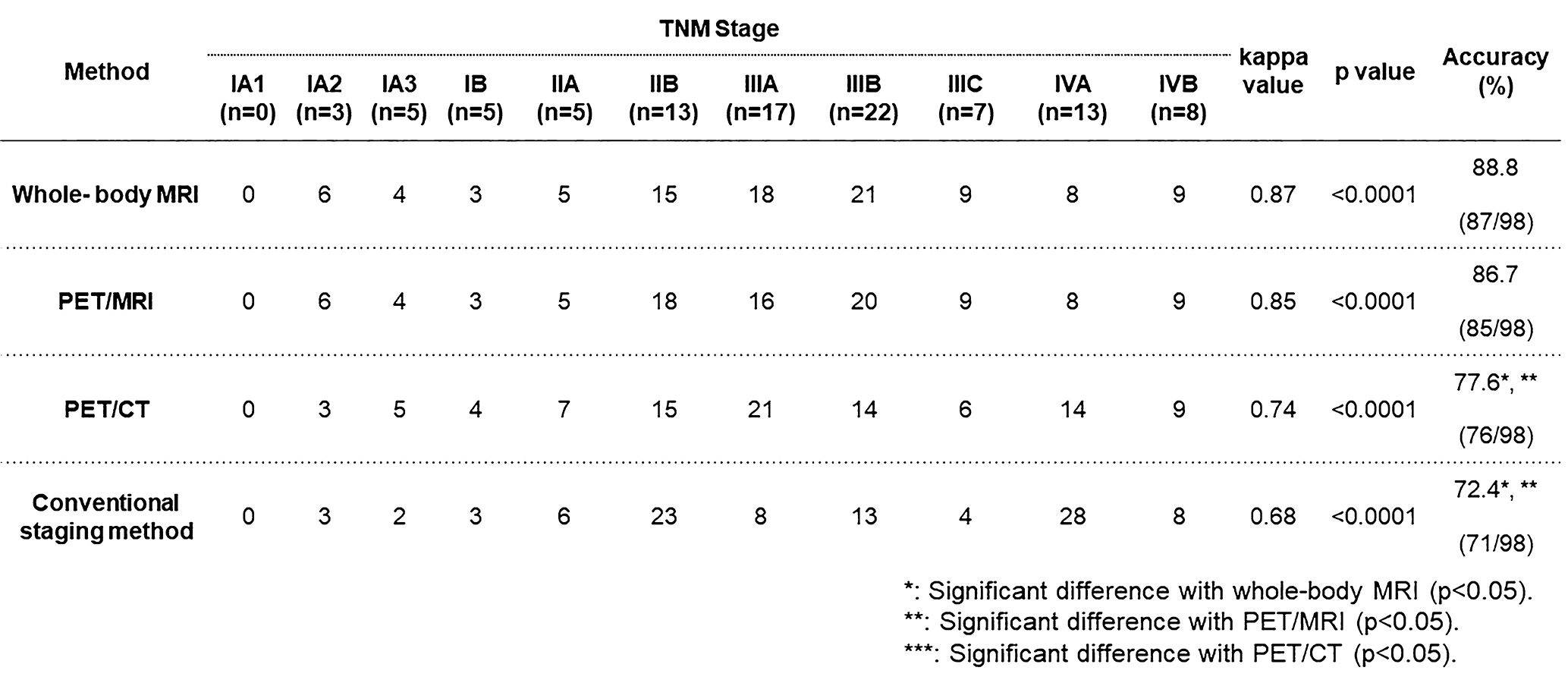
Figure 4. Agreements and diagnostic accuracy for TNM staging between final diagnosis and each method.
Agreement of each method determined as significant and substantial or almost perfect (0.68≤κ, p<0.0001). Moreover, accuracies of whole-body MRI and PET/MRI were significantly better than that of PET/CT and conventional staging method (p<0.05).

Figure 5. Agreements and diagnostic accuracy for VALSG staging between final diagnosis and each method.
Agreement of each method was determined as significant and almost perfect (0.83≤κ, p<0.0001). Moreover, accuracies of whole-body MRI and PET/MRI were significantly better than that of PET/CT and conventional staging method (p<0.05).