1413
Feasibility of real-time MRI of the actively moving wrist at 0.55 Tesla1Ming Hsieh Department of Electrical and Computer Engineering, University of Southern California, Los Angeles, CA, United States, 2Siemens Medical Solutions USA, Inc., Los Angeles, CA, United States, 3Orthopaedic Surgery, University of California Davis, Davis, CA, United States, 4Radiology, Stanford University School of Medicine, Stanford, CA, United States, 5Radiology, University of California Davis, Davis, CA, United States
Synopsis
In this work we show results from a first-in-human study utilizing a high-performance 0.55T system and balanced SSFP (bSSFP) real-time MRI acquisition to assess tissues of the actively moving wrist’s uninterrupted radial-ulnar deviation and clenched fist maneuvers. We show that at 0.55T, bSSFP is less sensitive to off-resonance and banding artifacts that frequently obscure critical wrist structures. We show that the high temporal resolution of 25 ms per frame at high-performance 0.55T enables improved characterization of wrist joint motion. These benefits could make it a promising technology to evaluate dynamic wrist instability.
INTRODUCTION
MRI is commonly employed in the evaluation of wrist pathology, including wrist instability, when X-ray findings are negative or uncertain. Standard MRI acquisition is however slow and precludes the adequate capture of the wrist during its motion, essential for evaluating dynamic wrist instability (DyWI). To address this shortcoming, real-time MRI (RT-MRI) protocols, typically using 3.0T scanners, have been developed for wrist imaging with temporal resolutions of up to 150-300 ms per slice1,2. However, these protocols are inadequate for assessing dynamic pathologies of interest in DyWI such as clunking, snapping, or clicking, and suffer from low signal-to-noise ratio and image artifacts that frequently obscure critical wrist structures. Recently, high-performance 0.55T MRI scanners have become available3 that have unique characteristics to overcome limitations of higher field strength systems for RT-MRI. We conducted a first-in-human study utilizing a high-performance 0.55T system and RT-MRI acquisition to assess tissues of the actively moving wrist during uninterrupted radial-ulnar deviation and clenched fist maneuvers.METHODS
Experiments: Experiments were performed using a whole-body 0.55T system (prototype MAGNETOM Aera, Siemens Healthineers, Erlangen, Germany) equipped with high-performance shielded gradients (45 mT/m amplitude, 200 T/m/s slew rate). This proof-of-concept study was approved by the institutional review board of the University of Southern California and written informed consent was obtained from all participants before the start of the study. The study cohort consisted of 3 asymptomatic participants (2 men, 1 woman). The dominant wrist for each participant was scanned. The participants lay in the “superman position” with one arm placed between a spine RF coil (below) and a 6-channel body coil (above), in a configuration that did not restrict wrist range of motion. Using the localizer acquisition, a coronal slice showing the scapholunate (SL) interval was prescribed. Each participant performed two wrist maneuvers relevant to evaluation for dynamic SL instability – radial-ulnar deviation and clenched fist maneuvers – during RT-MRI acquisition utilizing their full, active range-of-motion at their natural speed.Acquisition and Reconstruction: A 2D spiral balanced steady-state free-precession (bSSFP) sequence was implemented within the RTHawk real‐time imaging platform (HeartVista, Inc., Los Altos, CA, USA). Imaging parameters were: in-plane resolution = 1.38 x 1.38 mm2, slice thickness = 8 mm, field-of-view = 18 x 18 cm2, TR / TE= 12.70 / 0.78 ms, readout duration = 8.38 ms, sampling interval = 2 µs. Based on Bloch simulation of the bSSFP signal, we chose a flip angle of 70º that maximizes the signal from bone marrow fat tissue at 0.55T. We used a 13 spiral-out sampling scheme and temporal bit-reversed orders of spiral interleaves. Localization, imaging, and on-the-fly reconstructions were performed using the real-time console while MRI data were analyzed from off-line reconstructed images. We used a temporal finite-difference constrained reconstruction implemented using the Berkeley Advanced Reconstruction Toolbox4. Gradient impulse response function5,6 was estimated from a phantom-based measurement7 and used to correct spiral k-space trajectories, which are otherwise distorted due to the eddy current.
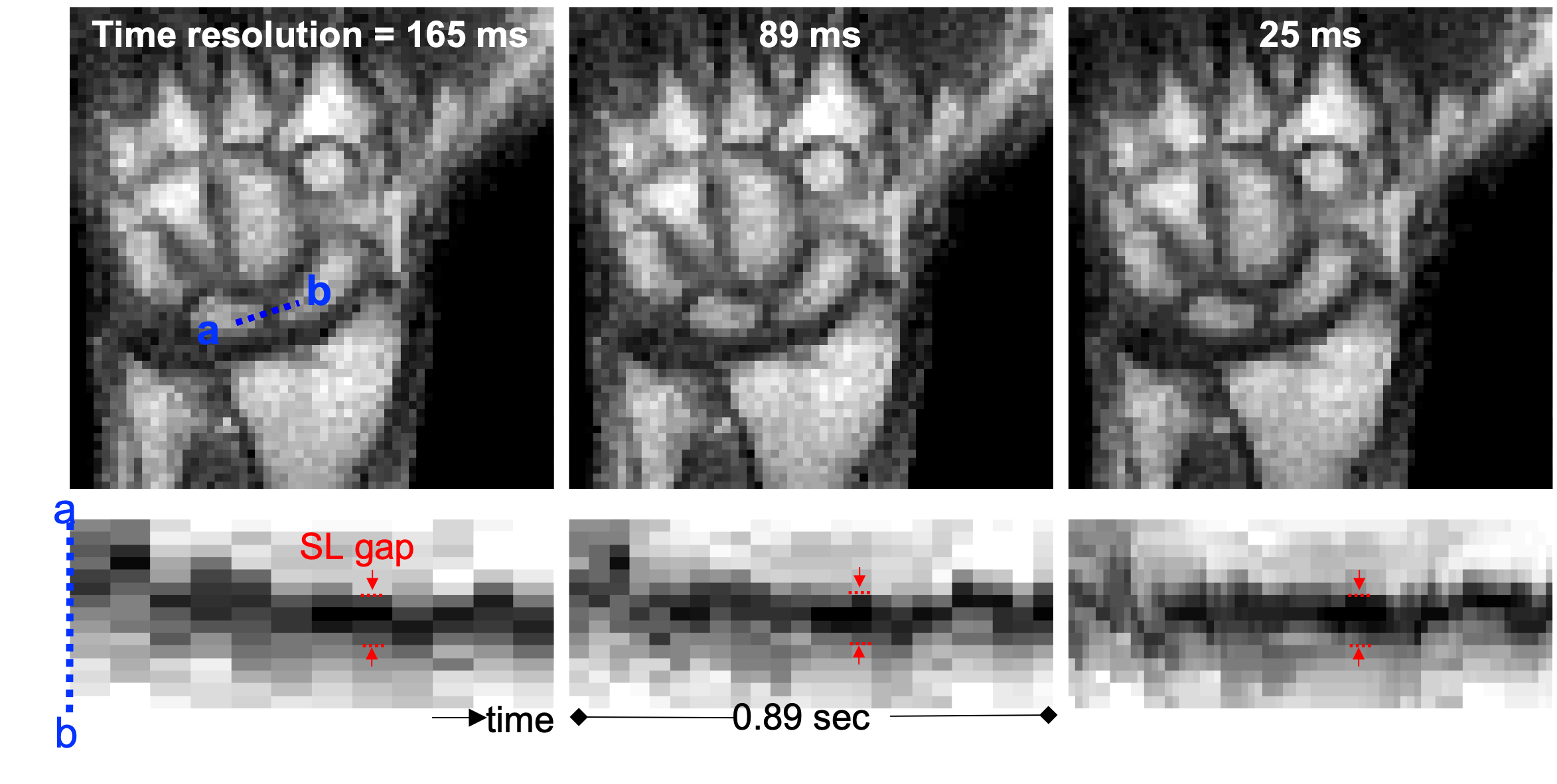
Analysis: From the reconstructed images, the image intensity vs. time plots through the middle of the SL interval were created. Change in the SL interval over time was evaluated for the various nominal temporal resolutions.
RESULTS
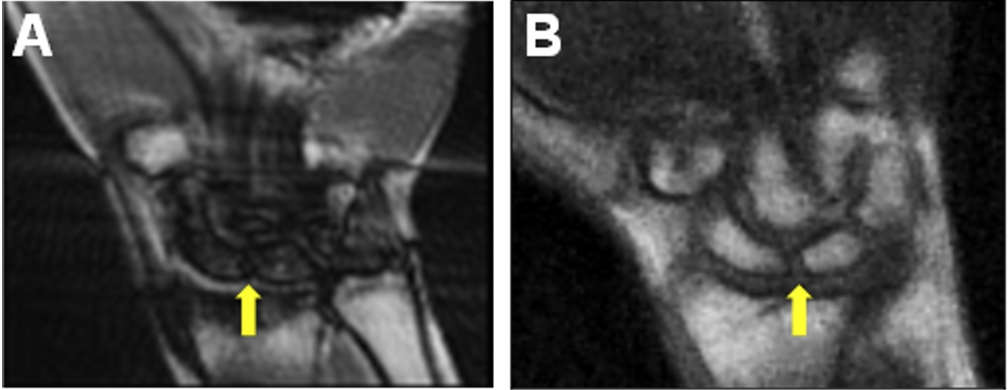
The bSSFP RT-MRI acquisitions of the moving wrist at 3.0T from previous publications showed characteristic banding artifacts that obscured the wrist anatomy of interest (Figure 1A)1. The bSSFP RT-MRI at 0.55T demonstrates the absence of these artifacts and improved visualization of the SL interval (Figure 1B). The temporal resolution at 3.0T with Nyquist sampling was limited to over 470 ms per imaging slice, while at 0.55T full sampling was accomplished in 165 ms. In analyzing the impact of the acceleration of image acquisition (nominal temporal resolution down from 165 ms to 25 ms) on image quality, minimal image degradation was noted (Figure 2). With a temporal resolution of 25 ms, the image intensity vs. time plots through the SL interval showed reduced temporal blurring and a shaper boundary between the scaphoid and lunate, indicating an improved ability to quantify changes to the SL interval over the range of motion.DISCUSSION and CONCLUSION
These initial results demonstrate that RT-MRI acquisition during continuous, active, and uninterrupted wrist motion is feasible with a 0.55T system and presents anatomical information of relevance to the assessment of DyWI. The high temporal resolution of 25 ms enabled improved characterization of wrist joint motion. Note that this work did not use a dedicated local wrist coil. We expect a boost in SNR with such a dedicate coil8. The lower field is also more amenable to instrumentation in the bore such as equipment to support loaded movements. These benefits combined with other advantages of low-field imaging, such as the ability to image immediately adjacent to metallic implants, the improved safety profile in patients with implantable devices, and lower acoustic noise3 make it a promising technology to evaluate further for improving the assessment of DyWI. Limitations of the study include its proof-of-concept nature (the small sample size and the inability to assess changes in the flexion-extension axis), and inclusion only of participants without wrist pathology.Acknowledgements
We acknowledge grant support from the National Science Foundation (#1828736) and research support from Siemens Healthineers.References
1. Shaw CB, Foster BH, Borgese M, Boutin RD, Bateni C, Boonsri P, Bayne CO, Szabo RM, Nayak KS, Chaudhari AJ. Real-time three-dimensional MRI for the assessment of dynamic carpal instability. PLoS One. 2019;14(9):e0222704.
2. Nayak KS, Lim Y, Campbell-Washburn AE, Steeden J. Real-Time Magnetic Resonance Imaging. J Magn Reson Imaging. 2020; Early view. doi:10.1002/jmri.27411
3. Campbell-Washburn AE, Ramasawmy R, Restivo MC, Bhattacharya I, Basar B, Herzka DA, Hansen MS, Rogers T, Bandettini WP, McGuirt DR, et al. Opportunities in interventional and diagnostic imaging by using high-performance low-field-strength MRI. Radiology. 2019;293(2):384–393.
4. Tamir JI, Ong F, Cheng JY, Uecker M, Lustig M. Generalized Magnetic Resonance Image Reconstruction using The Berkeley Advanced Reconstruction Toolbox. Proc the ISMRM 2016 Data Sampling and Image Reconstruction Workshop. 2016;2486:9660006. doi:10.5281/zenodo.31907
5. Robison RK, Li Z, Wang D, Ooi MB, Pipe JG. Correction of B0 eddy current effects in spiral MRI. Magn Reson Med. 2019;81(4):2501–2513
6. Campbell-Washburn AE, Xue H, Lederman RJ, Faranesh AZ, Hansen MS. Real-time distortion correction of spiral and echo planar images using the gradient system impulse response function. Magn Reson Med. 2016;75(6):2278–2285.
7. Bruijnen T, Stemkens B, van den Berg CAT, Tijssen RHN. Prospective GIRF-based RF phase cycling to reduce eddy current-induced steady-state disruption in bSSFP imaging. Magn Reson Med. 2020;84(1):115–127.
8. Nordmeyer-Massner JA, De Zanche N, Pruessmann KP. Mechanically adjustable coil array for wrist MRI. Magn Reson Med. 2009;61(2):429–438.
Figures