1403
The value of Modulated Flip Angle in Refocused Imaging with Extended Echo Trains with Compressed Sensing (MATRIX) in Knee MRI Imaging1China-Japan Union Hospital of Jilin University, Changchun, China, 2Linyi People’s Hospital, Linyi, China, 3Central Research Institute, United Imaging Healthcare, Shanghai, China
Synopsis
Three-Dimensional (3D) sequence of magnetic resonance imaging (MRI) plays a critical role in musculoskeletal joints imaging; however, its long acquisition time limits the clinical application. In such condition, Compressed sensing (CS) is introduced to accelerate MRI during clinical practice. We aimed to investigate the feasibility of an isotropic 3D variable-flip-angle fast spin echo (FSE) sequence with CS technique (CS-MATRIX) compared to conventional 2D sequences on knee imaging.
Introduction:
Conventional 2D MRI imaging has been widely used in evaluating musculoskeletal injuries; However, their inherent disadvantages are widely reported including low resolution along slice selection direction, signal interferences between contiguous slices, and blood flow artifacts. As a crucial weight-bearing joint, knees are easily happened with a variety of injuries, including meniscus tears, crucial ligament tears, cartilage and bone injuries. Nevertheless, it is especially challenging to evaluate knee imaging than other musculoskeletal joints because of its complex anatomical structures, which require equally high in-plane resolution and slice thickness to depict the anatomical structures clearly and identify varying degrees of injuries, especially tears of menisci and crucial ligaments (1,2). In this study, an isotropic 3D variable-flip-angle fast spin echo (FSE) (MATRIX) sequence with compressed sensing (CS) technique (CS-MATRIX) was employed to evaluate knee imagingMethods:
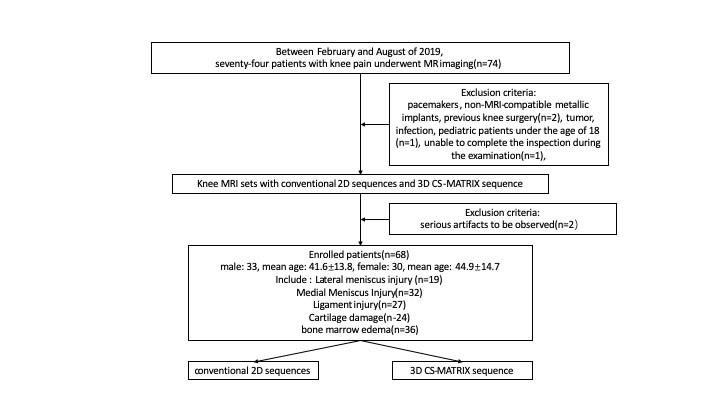
Patient Cohort:A total of seventy-four knees were enrolled. The flowchart of patient enrollment is summarized in Figure 1.MRI Protocols:All patients were examined with a 3.0 T MR scanner (uMR780, United Imaging Healthcare, Shanghai, China). MR imaging protocols included axial, sagittal and coronal 2D FSE T2-weighted fat-suppressed (T2-fs) and proton density-weighted non-fat-suppressed (pd-nfs) sequences. Image analysis: The signal-to-noise ratio (SNR) and contrast-to-noise ratio (CNR) of specific tissues were measured. Region-of-interests (ROIs) were manually drawn by the musculoskeletal radiologists. The radiologists were also enrolled to review the 68 examinations utilizing a four-point grading system to evaluate the image quality independently, according to the clarity of anatomical structures and imaging presence and severity of susceptibility or blood flow artefacts. Imaging qualities of medial menisci (MM), lateral menisci (LM), anterior cruciate ligament (ACL), posterior cruciate ligament (PCL) and cartilage–subchondral bone interface were assessed separately using the four-point image quality assessment system. The diagnostic agreement between the CS-MATRIX sequence and conventional sequences was also evaluated.Results:
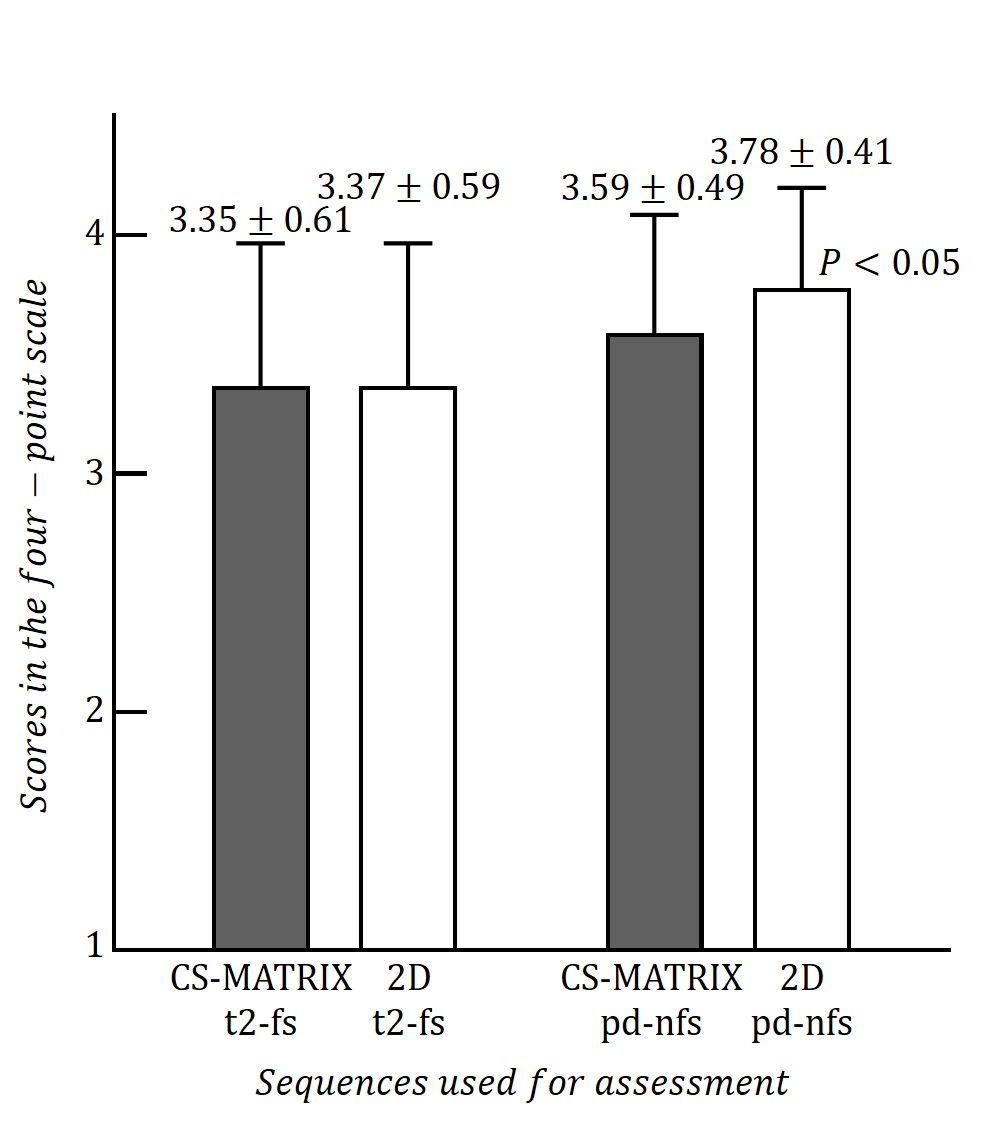
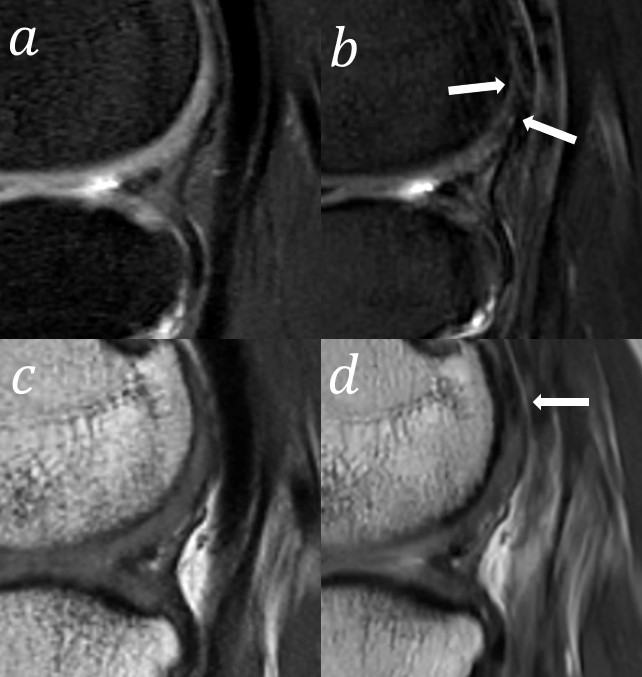
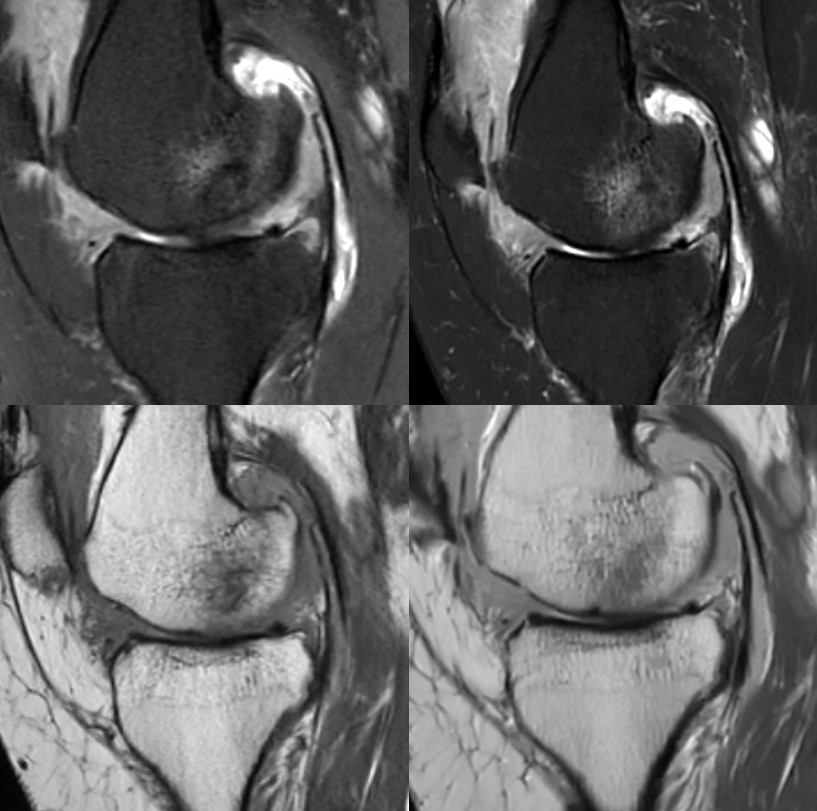
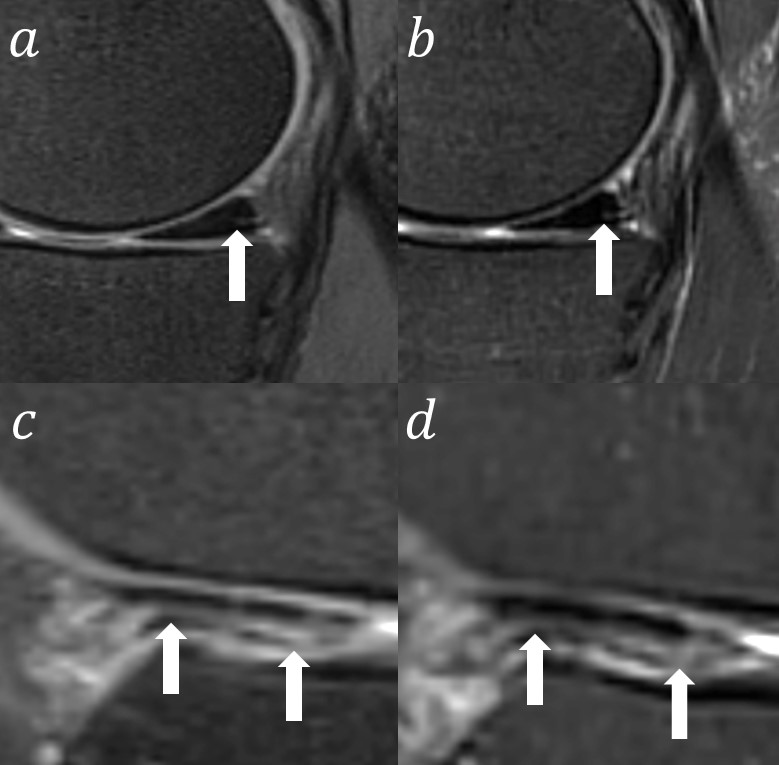
Images of T2-fs CS-MATRIX sequence had a significantly higher SNR than that of T2-fs 2D sequences in cartilage, menisci, and ligaments, and CNR of cartilage against both bone marrow and menisci calculated from T2-fs CS-MATRIX sequence were significantly higher than that of 2D T2-fs sequences. In addition, the CNR of synovial fluid against bone marrow and fat calculated from the CS-MATRIX sequence were significantly higher than those of the 2D sequences. The results of image quality comparisons are shown in Figure 2, no significant difference of image quality was found between T2-fs CS-MATRIX and T2-fs 2D sequences (mean score = 3.35±0.61 vs 3.37±0.59, p = 0.876), however, the image quality scores of pd-nfs 2D were significantly higher than those of pd-nfs CS-MATRIX sequence. CS-MATRIX sequence presents obviously improved image quality in blood flow artifacts reduction compared to conventional 2D sequences as shown in Figure 3. Diagnostic agreement analysis showed that there was a very good agreement between the isotropic CS-MATRIX and 2D sequences for detecting cartilage lesions (κ=1.000), and BMEs (κ=0.971). However, the range of the edemas shown in images from T2-fs CS-MATRIX sequence is not always as large as that of conventional T2-fs 2D sequences, and the contrast of edemas and surrounding normal bone marrow shown in pd-nfs CS-MATRIX images is better than that of pd-nfs 2D images (Figure 4). The diagnostic agreement reached good to very good in grading evaluation of MM and LM tears (κ=0.787, κ=0.910) (Figure 5).Discussion:
The results of this study demonstrated the successful application of an isotropic 3D variable-flip-angle FSE sequence with CS technique in knee MRI imaging, through various comparisons of CS-MATRIX with conventional 2D sequences. Previous investigations have demonstrated that 3D sequences could improve the diagnostic accuracy compared to conventional 2D sequences in comprehensive evaluations of knee joint injuries (3,4). Nonetheless, the isotropic spatial resolution and acquisition time are still remained to be optimized in clinical applications. Based on these considerations, CS technique came into the sight. In this study, with the advantages of both MATRIX sequence and CS technique, the accelerated isotropic T2-fs and pd-nfs CS-MATRIX sequences saved about 30% of total imaging time compared to the conventional 2D multi-planar sequences. In our study, with the presence of the additional nfs CS-MATRIX sequence, the diagnostic agreements of CL lesions and BME between the CS-MATRIX and conventional 2D sequences has reached good to very good. Additionally, marrow fat is known to present higher signals than edema in pd-nfs images, and lower signals while T2-fs sequences imaging. In clinical diagnosis, the smaller range of BME in images from T2-fs CS-MATRIX sequence may lead to false-negative diagnosis. On the contrary, the low signal in pd-nfs CS-MATRIX sequence could be mistakenly regarded as edema, which may lead to a false-positive judgement. Compared to the previous results, the combination of fs and nfs CS-MATRIX sequences is considered to have great potential in improving edema-related pathology detection, which is consistent with another study (5). In accordance with our expectation, the CS-MATRIX sequences yielded almost the same image quality as the conventional 2D sequences, even though the average subjective image quality score of pd-nfs CS-MATRIX sequence is slightly lower (5%) than it of pd-nfs 2D sequences.Conclusion:
In conclusion, this study demonstrates the clinical potential of MATRIX technique for knee imaging.Acknowledgements
NoneReferences
1. Wadhwa V, Omar H, Coyner K, Khazzam M, Robertson W, Chhabra A. ISAKOS classification of meniscal tears—illustration on 2D and 3D isotropic spin echo MR imaging. European Journal of Radiology 2016;85(1):15-24.
2. Yao L, Pitts JT, Thomasson D. Isotropic 3D fast spin-echo with proton-density-like contrast: a comprehensive approach to musculoskeletal MRI. AJR Am J Roentgenol 2007;188(2):W199-201.
3. Kudo H, Inaoka T, Kitamura N, et al. Clinical value of routine use of thin-section 3D MRI using 3D FSE sequences with a variable flip angle technique for internal derangements of the knee joint at 3T. Magn Reson Imaging 2013;31(8):1309-1317.
4. Ai T, Zhang W, Priddy NK, Li X. Diagnostic performance of CUBE MRI sequences of the knee compared with conventional MRI. Clin Radiol 2012;67(12):e58-63.
5. Cho HW, Suh JS, Park JO, et al. Three-Dimensional Fast Spin-Echo Imaging without Fat Suppression of the Knee: Diagnostic Accuracy Comparison to Fat-Suppressed Imaging on 1.5T MRI. Yonsei Med J 2017;58(6):1186-1194.
Figures