1401
Influence of group-oriented registration on functional ventilation parameters derived by 3D phase-resolved functional lung ventilation MRI1Institute of Diagnostic and Interventional Radiology, Hannover Medical School, Hannover, Germany, 2Biomedical Research in Endstage and Obstructive Lung Disease Hannover (BREATH), Member of the German Centre for Lung Research (DZL), Hannover, Germany, 3MR Application Predevelopment, Siemens Healthcare GmbH, Erlangen, Germany
Synopsis
Demonstration of a high repeatability is a mandatory step prior to the usage of new methods in clinical routine. Good to moderate repeatability of 3D phase-resolved functional lung (PREFUL) MRI was shown before. In this study, group-oriented registration (GOREG) was compared to stepwise registration regarding the repeatability of 3D PREFUL ventilation parameters in 30 study participants. Furthermore, image sharpness and structural similarity (SSIM) were assessed. An increased repeatability of dynamic 3D PREFUL ventilation parameters was observed using the GOREG approach. Also, image sharpness and SSIM values were significantly higher for measurements assessed with GOREG registration.
Introduction
Proton magnetic resonance 3D phase-resolved functional lung (PREFUL)1 and similar techniques2,3 provide contrast-free ventilation-weighted whole lung imaging by analyzing the signal of co-registered dynamic data of the lung during acquired during free breathing. Registration of lung images is challenging due to large deformations. As a solution, a stepwise registration or group-oriented image registration (GOREG)4 might help to avoid the need for large deformations between lung images and improve the registration accuracy. Recently, a good to moderate repeatability of 3D PREFUL ventilation parameters in healthy volunteers and chronic obstructive pulmonary disease (COPD) patients was reported using a stepwise registration to an inspiratory respiratory position5. In this study, our objective was to assess the influence of the GOREG and stepwise registration scheme on repeatability and image quality of 3D PREFUL ventilation parameters.Methods
20 healthy volunteers and 10 patients with COPD underwent MRI at 1.5T (MAGNETOM Avanto, Siemens Healthcare, Erlangen, Germany). Images were obtained during approximately 8 minute of free-breathing with a prototypical 3D stack-of-stars spoiled-gradient-echo sequence with golden-angle increment and following sequence parameters: FOV 50 x 50 cm2, TE/TR 0.81/1.9 msec, flip angle 3.5°, bandwidth 1500 Hz/pixel, matrix size 128 x 128, slice thickness 4 mm, final upsampled isotropical resolution 2 mm3. The acquisition was repeated for healthy volunteers after a break outside the scanner, and in median within 7 days [6-8 days] for COPD patients. After successful image reconstruction, registration towards the inspiratory image using the stepwise and GOREG registration, implemented in Advanced Normalization Tools (ANTs)6, was performed.The stepwise registration of approximately 40 phases was implemented, so that deformation fields are calculated for neighboring respiratory states in direction to end-inspiration (i.e. the 20th respiratory phase). Then, the deformation fields are used consecutively to register all images, e.g. for 1st respiratory phase, 19 deformations fields are applied in order to register 1st respiratory phase on 20th respiratory phase.
For the GOREG registration, the procedure is complemented by an additional registration step: intragroup registration. In the intragroup registration all images from one group are registered on reference image of the corresponding group. The averaged images of all groups are used for step-wise intergroup registration as described above. From the registered data, a regional ventilation (RVent) dynamic map with 16 respiratory phases was computed as previously described7. The RVent dynamics was analyzed by computing the regional flow-volume loops (FVL). Similarity of all FVLs to a healthy reference FVL, determined by RVent thresholding8, is evaluated using cross-correlation (CC). Ventilation defect percentage (VDP) maps were generated for RVent and CC (VDPRVent and VDPCC) using published thresholds1,5,9. Further, the RVent dynamics was assessed by generating ventilation time-to-peak (VTTP) maps in % deviation from the expected peak at full inspiration (50%):
$$VTTP_{Dev} = \:\mid VTTP - 50\%\: \mid\cdot$$
Differences were assessed with Wilcoxon signed rank tests and Pearson correlation analysis. Repeatability analysis included coefficient of variation (CoV), intraclass-correlation coefficient (ICC) and Bland-Altman plots. Furthermore, the image sharpness of RVent maps and mean structural similarity index (SSIM) of registered morphological images were computed.
Results
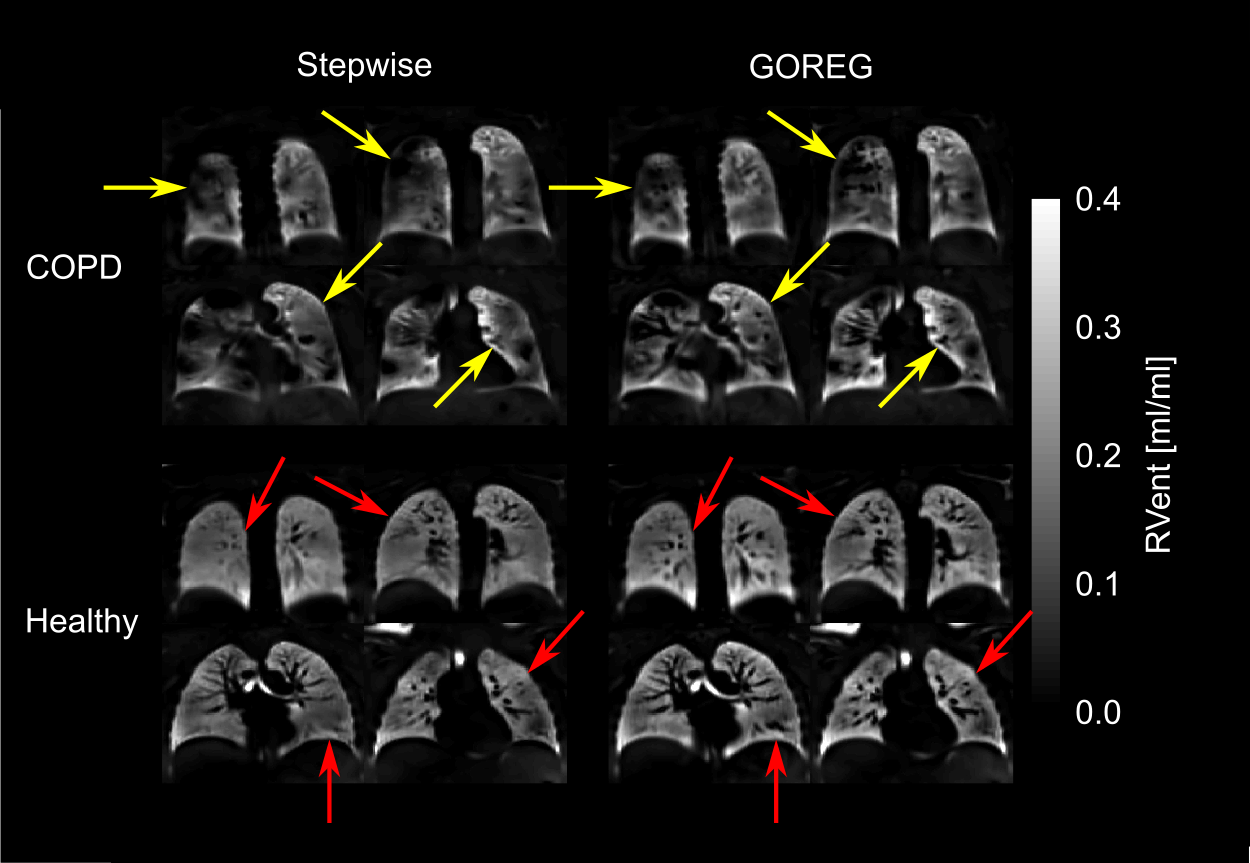
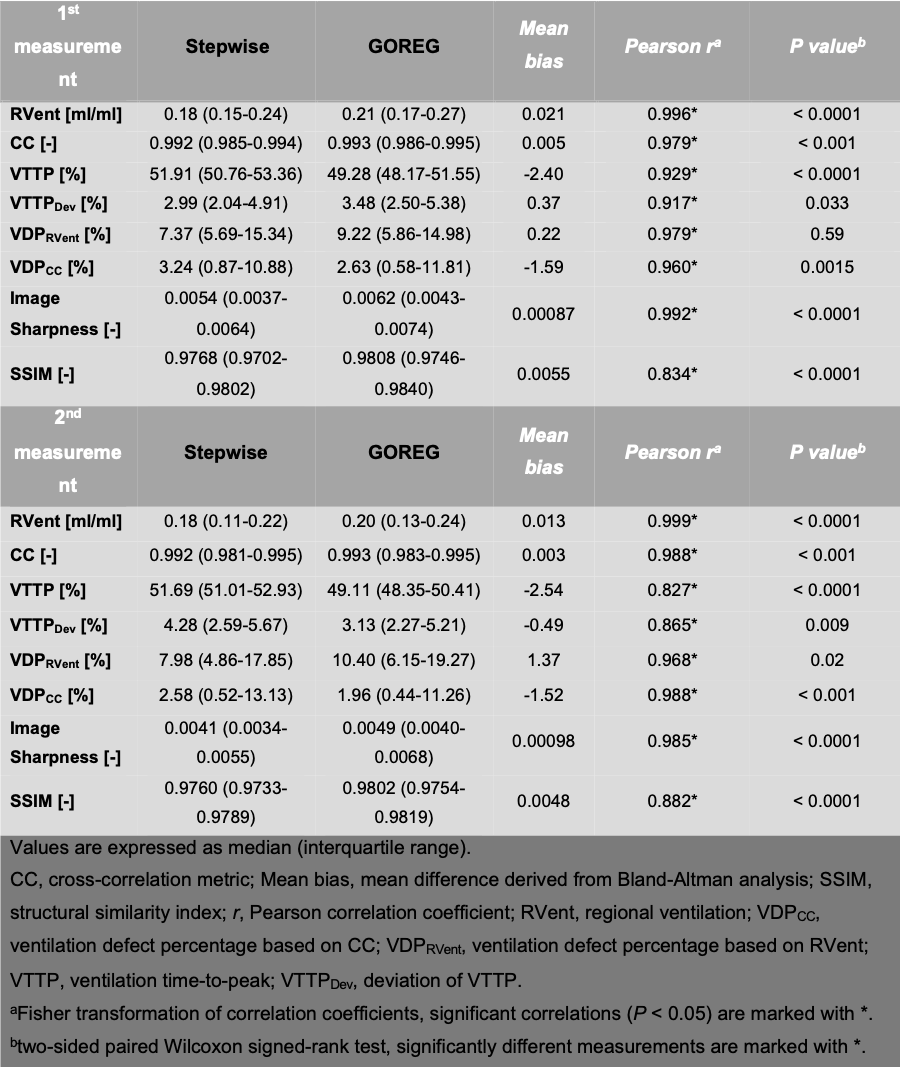
The median computing time was significantly different (P < 0.0001) between stepwise and GOREG approach (113 vs. 151 minutes per subject).Significant correlations (r range: 0.827-0.999, all P < 0.0001, Table 1) were observed between ventilation parameters, image sharpness and SSIM indices derived using both registration approaches in 1st and 2nd measurement comparison. This resulted in systematically higher RVvent values, increased CC values with GOREG registration as well as in significant VDP differences (Table 1).
Image sharpness values and SSIM indices were significantly increased for GOREG registration in both 3D PREFUL measurements (all P < 0.0001, Table 1, Figure 1).
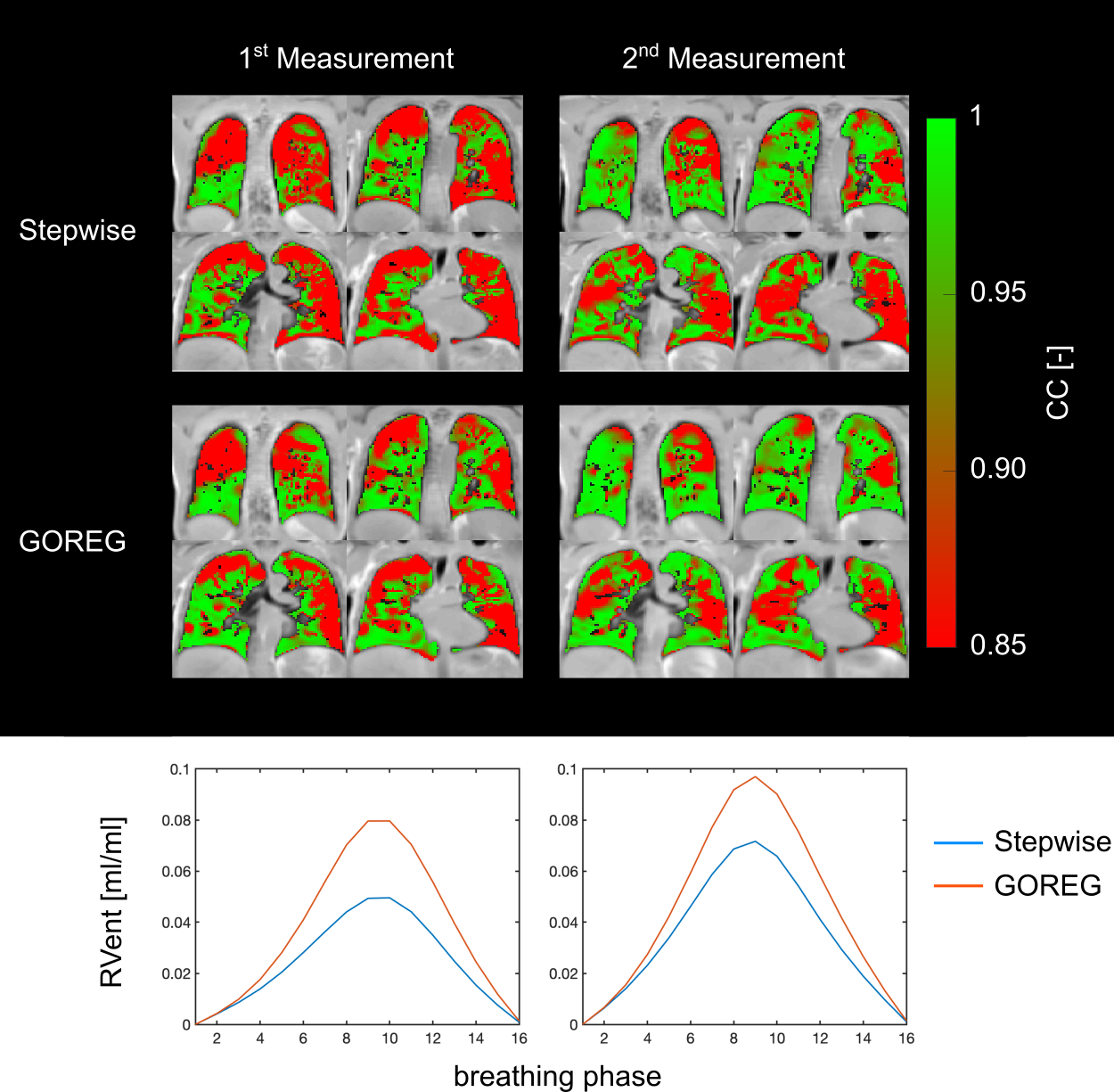
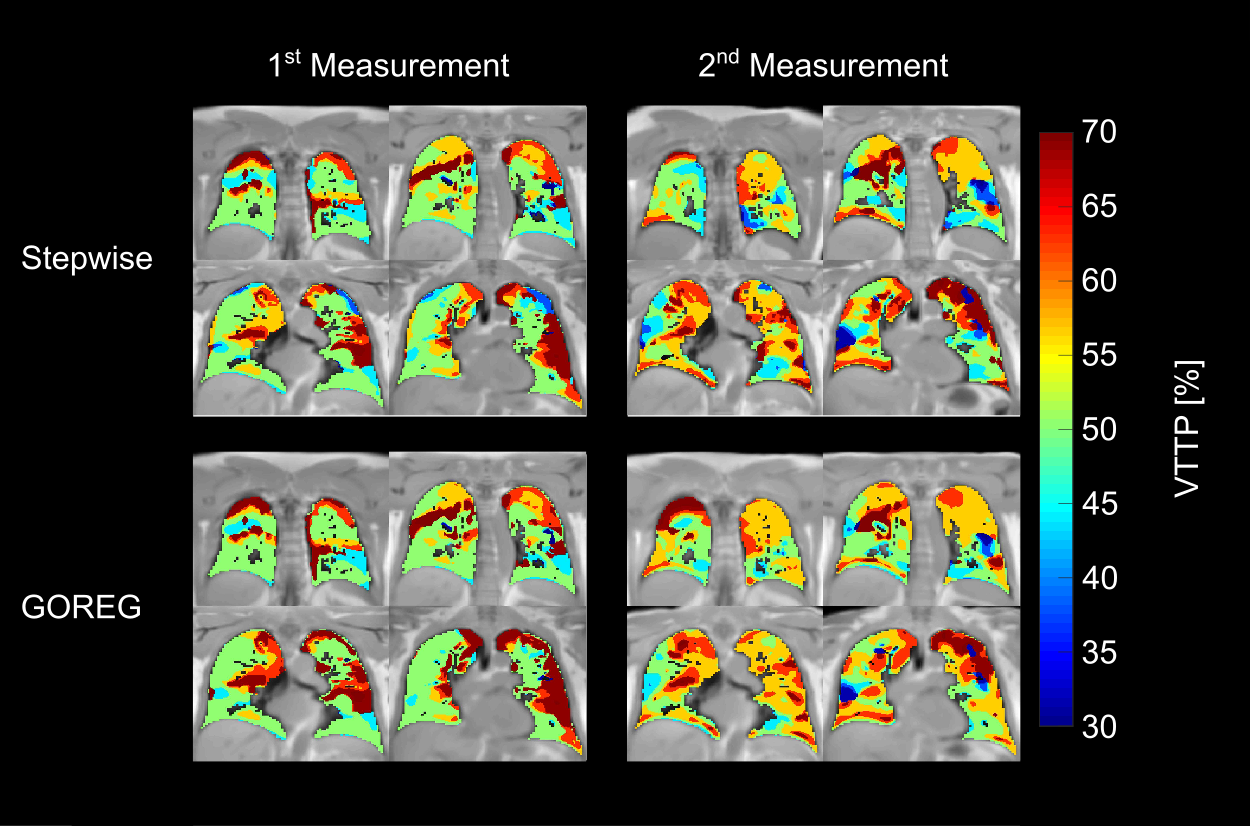
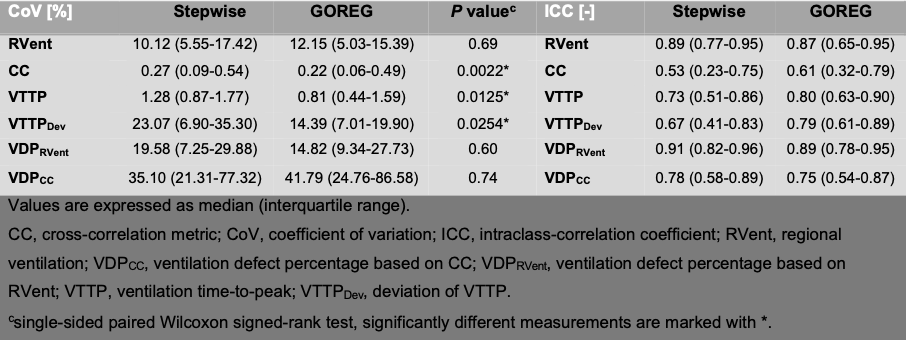
Regarding repeatability, median CoV values of CC, VTTP and VTTPDev parameters were significantly lower (all P < 0.0254, Table 2) for GOREG registration when compared to stepwise registation (see Table 2). Visual comparison of repeatability evaluation of COPD patients for both registration schemes is seen in Figure 2 for CC parameter and in Figure 3 for the VTTP parameter.
Discussion
Results of this work indicate that the repeatability of dynamic 3D PREFUL ventilation is significantly improved using GOREG registration and that the image sharpness of RVent maps is significantly increased.Repeatability analysis showed significantly decreased median CoV values and significantly increased ICC values of dynamic ventilation parameters (CC, VTTP and VTTPDev) for the GOREG registration scheme, when compared to stepwise registration. This fact suggests that the GOREG registration improves the accuracy of registration and repeatability of dynamic 3D PREFUL ventilation parameters. This can be explained by the increased parenchymal signal due to averaging several slices within each breathing group resulting in more accurate intergroup registration. Importantly, GOREG leads to systematically higher RVent ventilation values and higher VDPRVent likely due to the improved image quality compared to stepwise registration.
Similarly to previous 2D results4, the image sharpness of RVent ventilation maps and also SSIM index of GOREG registered morphological images was superior compared to stepwise registration. The drawback of GOREG registration is a longer computation time (~38 minutes per subject).
Conclusion
The GOREG registration approach improves the repeatability of dynamic 3D PREFUL ventilation parameters and results in superior image sharpness of RVent maps in comparison to stepwise registration.Acknowledgements
This work was supported by the German Centre for Lung Research (DZL). The authors thank Melanie Pfeifer and Frank Schröder for outstanding technical assistance in performing the MRI examinations.References
1. Klimeš F, Voskrebenzev A, Gutberlet M, et al. 3D phase‐resolved functional lung ventilation MR imaging in healthy volunteers and patients with chronic pulmonary disease. Magn Reson Med. 2021;85(2):912-925. doi:10.1002/mrm.28482
2. Boucneau T, Fernandez B, Larson P, Darrasse L, Maître X. 3D Magnetic Resonance Spirometry. Sci Rep. 2020;10(1):1-12. doi:10.1038/s41598-020-66202-7
3. Mendes Pereira L, Wech T, Weng AM, et al. UTE-SENCEFUL: first results for 3D high-resolution lung ventilation imaging. Magn Reson Med. 2018;(August):1-10. doi:10.1002/mrm.27576
4. Voskrebenzev A, Gutberlet M, Kaireit TF, Wacker F, Vogel-Claussen J. Low-pass imaging of dynamic acquisitions (LIDA) with a group-oriented registration (GOREG) for proton MR imaging of lung ventilation. Magn Reson Med. 2017;78(4):1496-1505. doi:10.1002/mrm.26526
5. Klimeš F, Voskrebenzev A, Gutberlet M, et al. Repeatability of dynamic 3D phase-resolved functional lung (PREFUL) ventilation MR Imaging in patients with chronic obstructive pulmonary disease and healthy volunteers. J Magn Reson Imaging. 2021;54(2):618-629. doi:10.1002/jmri.27543
6. Avants BB, Tustison NJ, Song G, Cook PA, Klein A, Gee JC. A reproducible evaluation of ANTs similarity metric performance in brain image registration. Neuroimage. 2011;54(3):2033-2044. doi:10.1016/j.neuroimage.2010.09.025
7. Klimeš F, Voskrebenzev A, Gutberlet M, et al. Free‐breathing quantification of regional ventilation derived by phase‐resolved functional lung (PREFUL) MRI. NMR Biomed. 2019;(February):e4088. doi:10.1002/nbm.4088
8. Moher Alsady T, Voskrebenzev A, Greer M, et al. MRI‐derived regional flow‐volume loop parameters detect early‐stage chronic lung allograft dysfunction. J Magn Reson Imaging. 2019;L:1-10. doi:10.1002/jmri.26799
9. Pöhler GH, Klimeš F, Behrendt L, et al. Repeatability of Phase‐Resolved Functional Lung (PREFUL)‐ MRI Ventilation and Perfusion Parameters in Healthy Subjects and COPD Patients. J Magn Reson Imaging. October 2020:jmri.27385. doi:10.1002/jmri.27385
Figures