1394
Three-fold accelerated MRI and MR angiography on Moyamoya disease examination using deep learning constrained Compressed SENSE reconstruction1BU-MR Clinical Science, Philips Healthcare, Suzhou, China, 2Philips Healthcare, Shanghai, China, 3Department of Radiology, Nanjing Drum Tower Hospital, The Affiliated Hospital of Nanjing University Medical School, Nanjing, China, 4BU-MR Clinical Science, Philips Healthcare, Best, Netherlands, 5BU-MR Clinical Science, Philips Healthcare, Tokyo, Japan
Synopsis
MR angiography (MRA) in moyamoya disease has been uniquely important in the evaluation of changes in vasculature and brain parenchyma, and clinical follow-up. In this work, we investigate the performance of accelerated MRA under a deep learning constrained Compressed SENSE reconstruction framework. Results on both volunteer and patients demonstrate a three-fold scan acceleration against the routine MRA with comparable image quality.
Introduction
Moyamoya disease (MMD) is a rare progressive cerebrovascular disease caused by arterial obstruction in the basal part of the brain1, and MRI and MR angiography (MRA) are reliable and noninvasive methods for MMD diagnosis with excellent diagnostic yield. However, the clinical routine MRA is time-consuming which brings increased chance of scan failure due to patients’ discomfort and movement. Recently, the Adaptive-CS-Net deep learning method2 was introduced and integrated in Compressed SENSE (CS) for MRI reconstruction (called CS-AI hereafter), and superior performance has been reported on various anatomical applications such as shoulder3, prostate4 and cardiac imaging5. In this study, we investigate the performance of CS-AI reconstruction on healthy volunteer and MMD patients, and compare with SENSE and CS images with respect to image quality and scanning efficiency.Methods
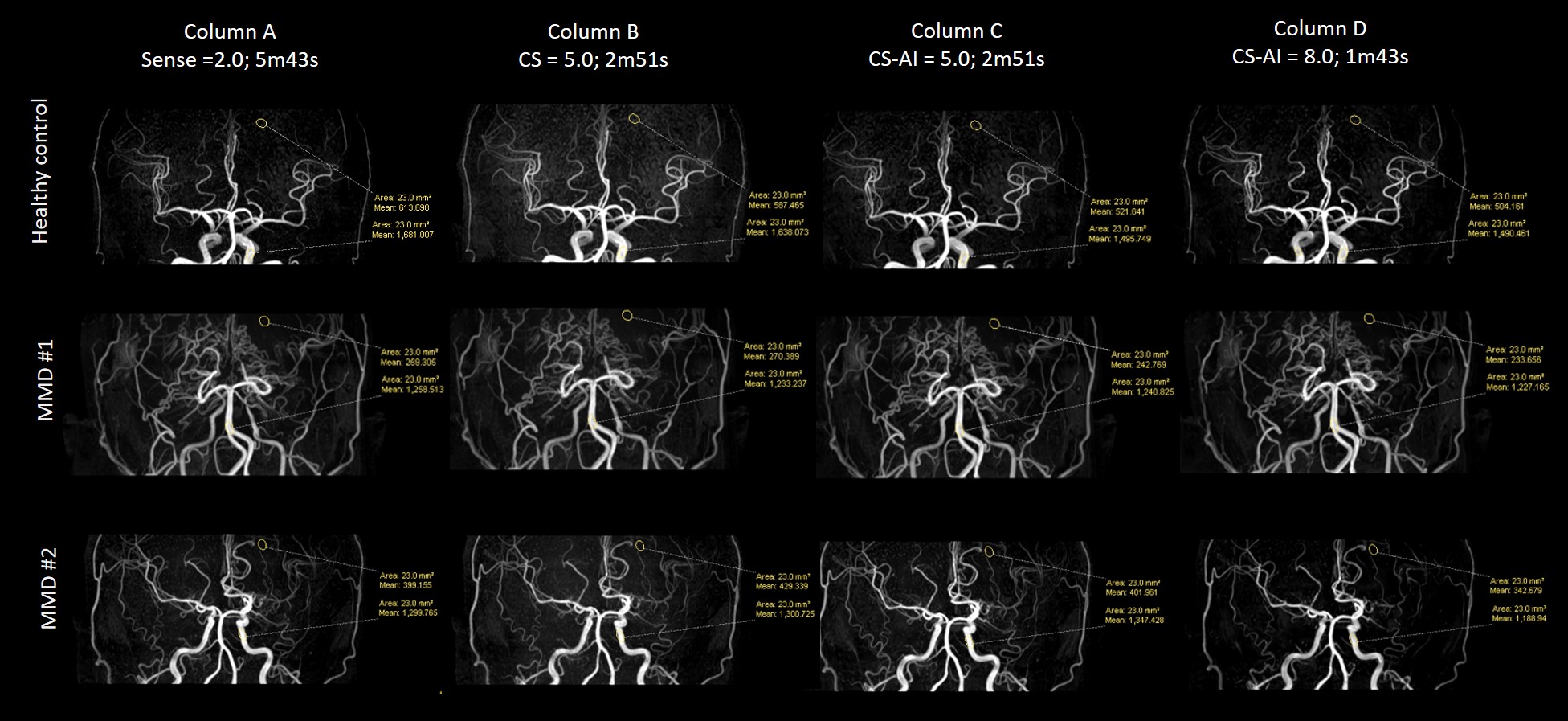
The MR imaging was performed on an Ingenia CX 3.0 T system (Philips Healthcare, the Netherlands) with one volunteer and two MMD patients under written informed consent. The 32-channel head array coil was used to acquire the anatomical 3D T1w, multi-slice T2w, 3D FLAIR and 3D TOF-MRA images. The scanning parameters, including TE/TR, FOV, voxel size, slice thickness, acceleration schemes and scan times are listed in Table 1. For the scan acceleration factors, we used SENSE factor s=2 as a baseline (as empirical clinical routine MRA setting), and repeated the scans using different CS factors (listed in Table 1). The data acquired from SENSE and CS acquisitions were reconstructed using their default reconstruction methods. In addition, the CS data was also reconstructed using the Adaptive-CS-Net neural network model 2.In the routine MRA (SENSE factor = 2) vessel views, for each subject two ROIs of equal area were manually delineated on the vertebral artery (ROI#1) and on a region in the brain without visible vessels (ROI#2), respectively. Examples of the ROI placement are shown in Figure 1. The ROIs were then mapped to the CS and CS-AI images of the same subject. The vessel contrast to noise ratio (CNR) was calculated by $$$(SI\_mean_{ROI1}-SI\_mean_{ROI2}) / SI\_stdev_{ROI2}$$$, where SI stands for the signal intensity. This serves as a marker of the imaging contrast of the vessels against the background noise (vessel-to-noise). This ratio was compared for SENSE =2.0, CS = 5.0, CS-AI = 5.0 and CS-AI = 8.0 for MRA.
Results
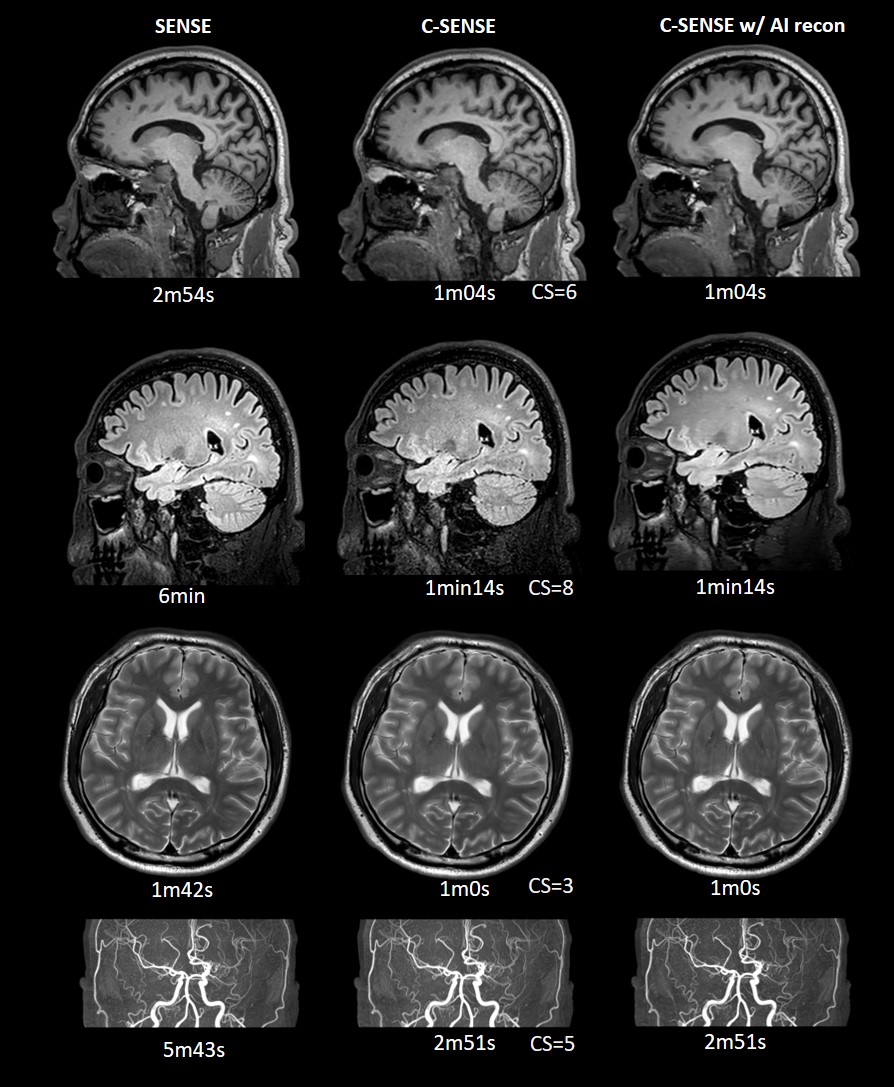
Figure 1 compares the MRA images with different acceleration factors and reconstructions. From the scans with acceleration factor 5, CS-AI (column C) has better background suppression compared to CS (column B) only. CS-AI 8 allowed to reduce the scan time to 1m43s, achieving a 3-fold acceleration against baseline MR while maintaining image quality. The ROI intensity ratios shown in Table 2 also demonstrate that CS-AI 5 and CS-AI 8 provided superior vessel-to-noise ratio than CS 5 and the baseline. Figure 2 demonstrates a clinical routine imaging set for MMD patient examinations. The total scan time for the baseline protocol set was 16m19s. The following acceleration factors for each imaging contrast were used: CS-AI = 6.0 for 3D T1w, CS-AI = 3.0 for multi-slice T2w, CS-AI = 8.0 for 3D FLAIR and CS-AI = 5.0 for MRA. The resulting images (Fig.3-right column) provided similar image quality compared to the baseline scans. The total scan time was brought back to 6m9s.Discussion and Conclusion
MRA for MMD patients is very important for surgery decisions and distal vessels evaluation. We have demonstrated 3-fold accelerated MRA imaging on moyamoya disease examinations using CS-AI reconstructions which is not affecting the imaging quality and diagnosis confidence. For moyamoya routine scans, the CS-AI scheme can also be applied to imaging contrasts of 3D T1w, multi-slice T2w, 3D FLAIR and MRA, dramatically reducing the total examination time. The CS-AI scheme needs to be further validated with large sample clinical cases for accelerating routine neuro MRI examinations.Acknowledgements
No.References
1. Fujimura M, Bang OY, Kim JS. Moyamoya Disease. Front Neurol Neurosci. 2016; 40: 204-220. doi: 10.1159/000448314.
2. Pezzotti N , Yousefi S , MS Elmahdy, et al. An Adaptive Intelligence Algorithm for Undersampled Knee MRI Reconstruction: Application to the 2019 fastMRI Challenge[J]. 2020.
3. J. Kwon M. et al. Ultrafast motion-minimized shoulder MRI with a deep learning constrained Compressed SENSE reconstruction. ISMRM 2021.
4. M. Yoneyama, et al. Rapid submillimeter high-resolution prostate T2 mapping with a deep learning constrained Compressed SENSE reconstruction. ISMRM 2021.
5. K. Yuda, et al. Myocardial T2-weighted black-blood imaging with a deep learning constrained Compressed SENSE reconstruction. ISMRM 2021.
Figures